

Chromosomal instability confers intrinsic multidrug resistance
- PMID: 21363922
- PMCID: PMC3059493
- DOI: 10.1158/0008-5472.CAN-10-3604
Chromosomal instability confers intrinsic multidrug resistance
Abstract
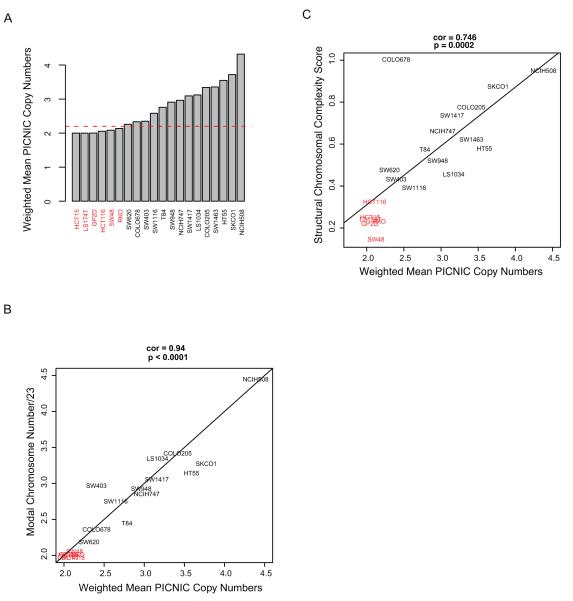
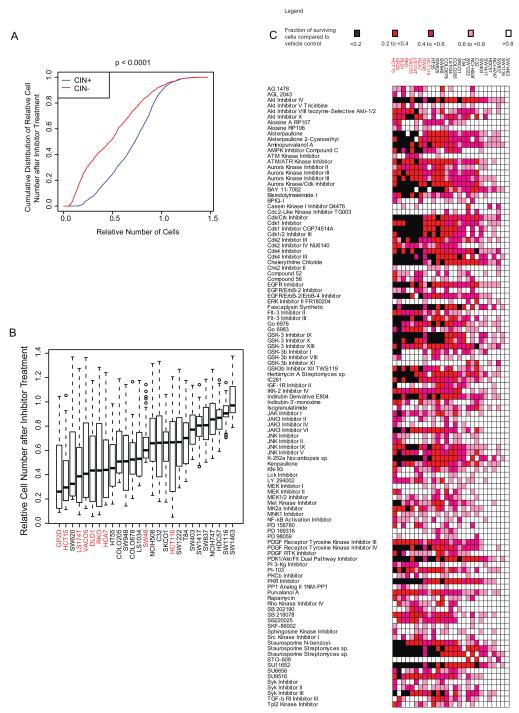
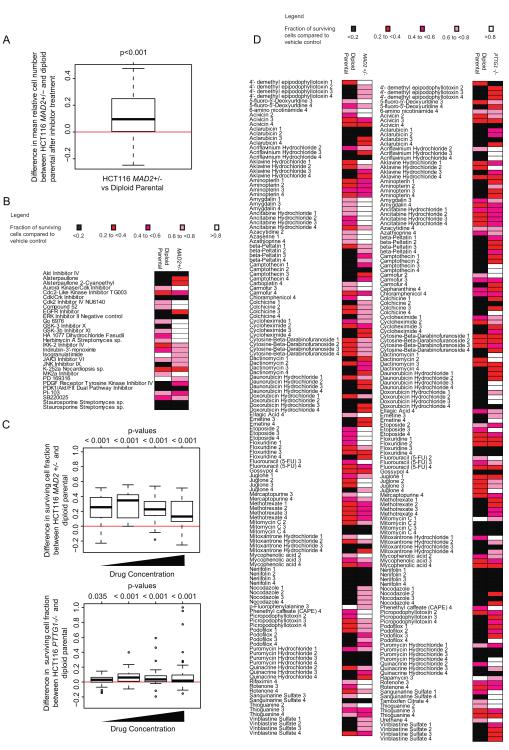
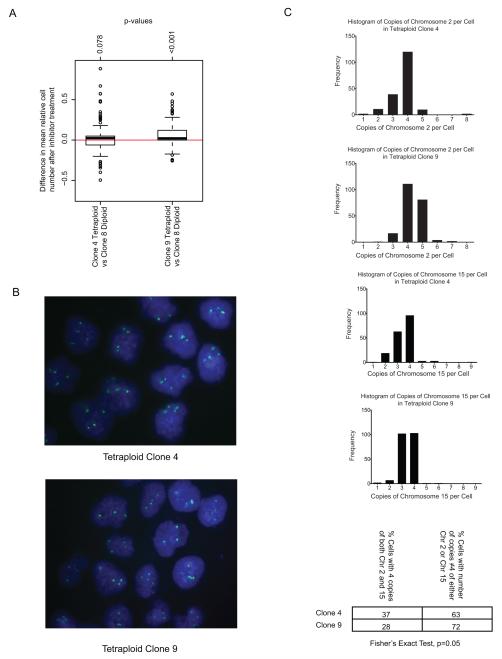
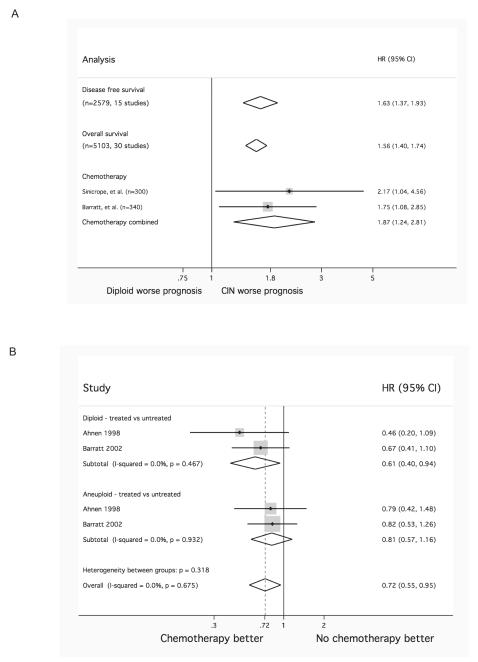
Aneuploidy is associated with poor prognosis in solid tumors. Spontaneous chromosome missegregation events in aneuploid cells promote chromosomal instability (CIN) that may contribute to the acquisition of multidrug resistance in vitro and heighten risk for tumor relapse in animal models. Identification of distinct therapeutic agents that target tumor karyotypic complexity has important clinical implications. To identify distinct therapeutic approaches to specifically limit the growth of CIN tumors, we focused on a panel of colorectal cancer (CRC) cell lines, previously classified as either chromosomally unstable (CIN(+)) or diploid/near-diploid (CIN(-)), and treated them individually with a library of kinase inhibitors targeting components of signal transduction, cell cycle, and transmembrane receptor signaling pathways. CIN(+) cell lines displayed significant intrinsic multidrug resistance compared with CIN(-) cancer cell lines, and this seemed to be independent of somatic mutation status and proliferation rate. Confirming the association of CIN rather than ploidy status with multidrug resistance, tetraploid isogenic cells that had arisen from diploid cell lines displayed lower drug sensitivity than their diploid parental cells only with increasing chromosomal heterogeneity and isogenic cell line models of CIN(+) displayed multidrug resistance relative to their CIN(-) parental cancer cell line derivatives. In a meta-analysis of CRC outcome following cytotoxic treatment, CIN(+) predicted worse progression-free or disease-free survival relative to patients with CIN(-) disease. Our results suggest that stratifying tumor responses according to CIN status should be considered within the context of clinical trials to minimize the confounding effects of tumor CIN status on drug sensitivity.
©2011 AACR.
Figures
References
-
- Lengauer C, Kinzler KW, Vogelstein B. Genetic instabilities in human cancers. Nature. 1998;396:643–9. - PubMed
-
- Lengauer C, Kinzler KW, Vogelstein B. Genetic instability in colorectal cancers. Nature. 1997;386:623–7. - PubMed
-
- Roschke AV, Tonon G, Gehlhaus KS, et al. Karyotypic complexity of the NCI-60 drug-screening panel. Cancer Res. 2003;63:8634–47. - PubMed
-
- Lothe RA, Peltomaki P, Meling GI, et al. Genomic instability in colorectal cancer: relationship to clinicopathological variables and family history. Cancer Res. 1993;53:5849–52. - PubMed
-
- Thibodeau SN, French AJ, Cunningham JM, et al. Microsatellite instability in colorectal cancer: different mutator phenotypes and the principal involvement of hMLH1. Cancer Res. 1998;58:1713–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
