

Antihypertensive treatment and secondary prevention of cardiovascular disease events among persons without hypertension: a meta-analysis
- PMID: 21364140
- PMCID: PMC4313888
- DOI: 10.1001/jama.2011.250
Antihypertensive treatment and secondary prevention of cardiovascular disease events among persons without hypertension: a meta-analysis
Erratum in
- JAMA. 2011 May 11;305(18):1862
Abstract
Context: Cardiovascular disease (CVD) risk increases beginning at systolic blood pressure levels of 115 mm Hg. Use of antihypertensive medications among patients with a history of CVD or diabetes and without hypertension has been debated.
Objective: To evaluate the effect of antihypertensive treatment on secondary prevention of CVD events and all-cause mortality among persons without clinically defined hypertension.
Data sources: Meta-analysis with systematic search of MEDLINE (1950 to week 3 of January 2011), EMBASE, and the Cochrane Collaboration Central Register of Controlled Clinical Trials and manual examination of references in selected articles and studies.
Study selection: From 874 potentially relevant publications, 25 trials that fulfilled the predetermined inclusion and exclusion criteria were included in the meta-analysis.
Data extraction: Information on participant characteristics, trial design and duration, treatment drug, dose, control, and clinical events were extracted using a standardized protocol. Outcomes included stroke, myocardial infarction (MI), congestive heart failure (CHF), composite CVD outcomes, CVD mortality, and all-cause mortality.
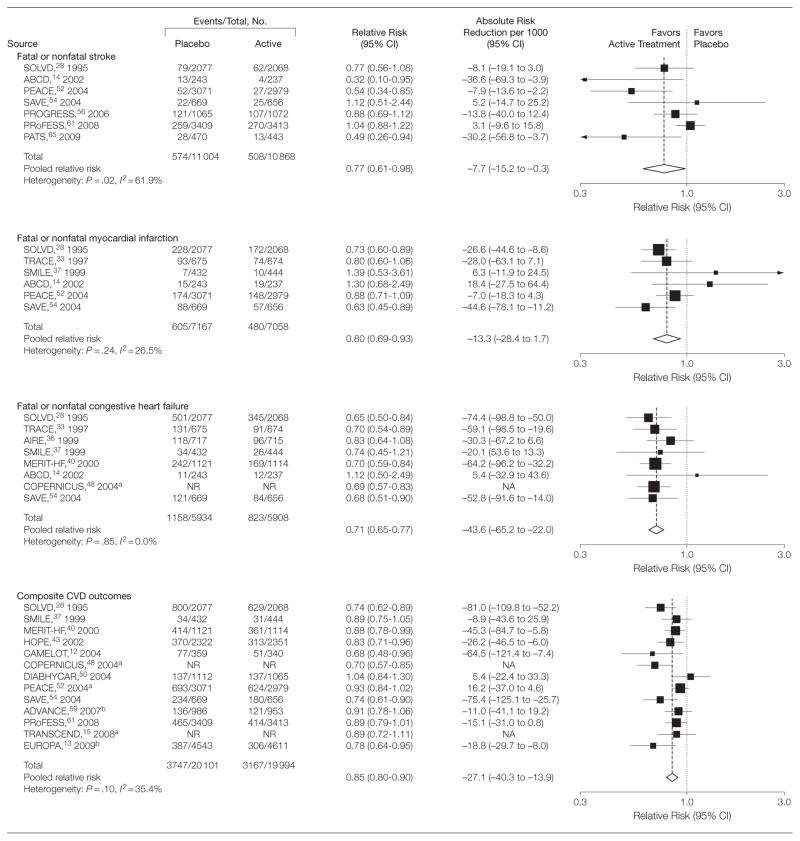
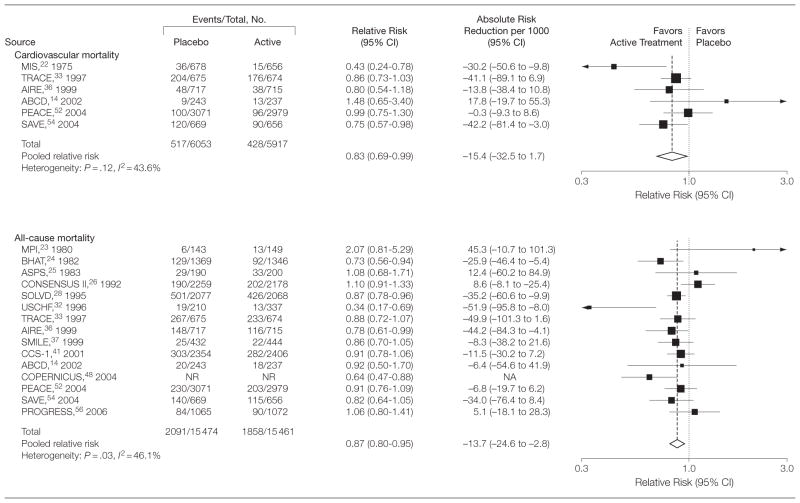
Results: Compared with controls, participants receiving antihypertensive medications had a pooled relative risk of 0.77 (95% confidence interval [CI], 0.61 to 0.98) for stroke, 0.80 (95% CI, 0.69 to 0.93) for MI, 0.71 (95% CI, 0.65 to 0.77) for CHF, 0.85 (95% CI, 0.80 to 0.90) for composite CVD events, 0.83 (95% CI, 0.69 to 0.99) for CVD mortality, and 0.87 (95% CI, 0.80 to 0.95) for all-cause mortality from random-effects models. The corresponding absolute risk reductions per 1000 persons were -7.7 (95% CI, -15.2 to -0.3) for stroke, -13.3 (95% CI, -28.4 to 1.7) for MI, -43.6 (95% CI, -65.2 to -22.0) for CHF events, -27.1 (95% CI, -40.3 to -13.9) for composite CVD events, -15.4 (95% CI, -32.5 to 1.7) for CVD mortality, and -13.7 (95% CI, -24.6 to -2.8) for all-cause mortality. Results did not differ according to trial characteristics or subgroups defined by clinical history.
Conclusions: Among patients with clinical history of CVD but without hypertension, antihypertensive treatment was associated with decreased risk of stroke, CHF, composite CVD events, and all-cause mortality. Additional randomized trial data are necessary to assess these outcomes in patients without CVD clinical recommendations.
Conflict of interest statement
Figures

Comment in
-
Antihypertensive therapy for prehypertension: relationship with cardiovascular outcomes.JAMA. 2011 Mar 2;305(9):940-1. doi: 10.1001/jama.2011.256. JAMA. 2011. PMID: 21364146 No abstract available.
-
Antihypertensive treatment of patients with cardiovascular disease but without hypertension.JAMA. 2011 Jun 1;305(21):2170-1; author reply 2171. doi: 10.1001/jama.2011.705. JAMA. 2011. PMID: 21632478 No abstract available.
-
Antihypertensive treatment of patients with cardiovascular disease but without hypertension.JAMA. 2011 Jun 1;305(21):2170; author reply 2171. doi: 10.1001/jama.2011.704. JAMA. 2011. PMID: 21632479 No abstract available.
-
ACP Journal Club. Review: Antihypertensive treatment prevents cardiovascular events and mortality in cardiovascular disease without hypertension.Ann Intern Med. 2011 Jun 21;154(12):JC6-6. doi: 10.7326/0003-4819-154-12-201106210-02006. Ann Intern Med. 2011. PMID: 21690584 No abstract available.
References
-
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet. 1997;349(9064):1498–1504. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, et al. Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42(6):1206–1252. - PubMed
-
- Lawes CM, Vander Hoorn S, Rodgers A International Society of Hypertension. Global burden of blood-pressure-related disease, 2001. Lancet. 2008;371 (9623):1513–1518. - PubMed
-
- Greenlund KJ, Croft JB, Mensah GA. Prevalence of heart disease and stroke risk factors in persons with prehypertension in the United States, 1999–2000. Arch Intern Med. 2004;164(19):2113–2118. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
