

Time to diagnosis and mortality in colorectal cancer: a cohort study in primary care
- PMID: 21364593
- PMCID: PMC3065288
- DOI: 10.1038/bjc.2011.60
Time to diagnosis and mortality in colorectal cancer: a cohort study in primary care
Erratum in
- Br J Cancer. 2011 Jun 7;104(12):1930
Abstract
Background: The relationship between the diagnostic interval and mortality from colorectal cancer (CRC) is unclear. This association was examined by taking account of important confounding factors at the time of first presentation of symptoms in primary care.
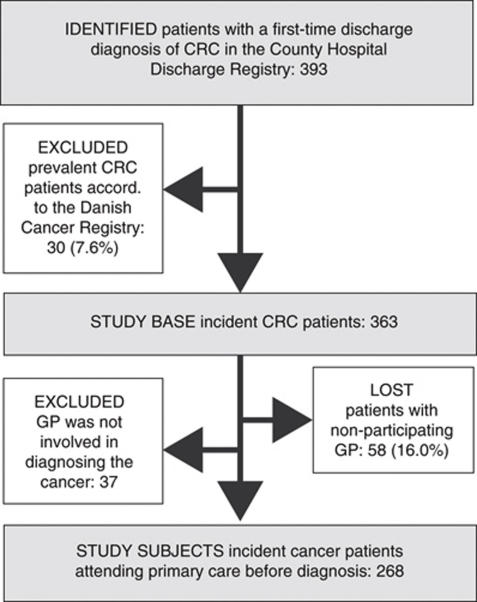
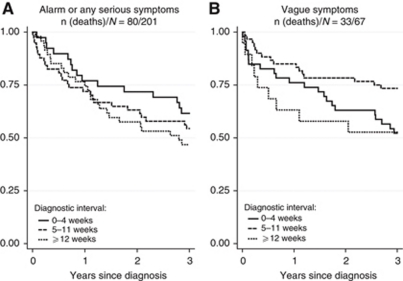
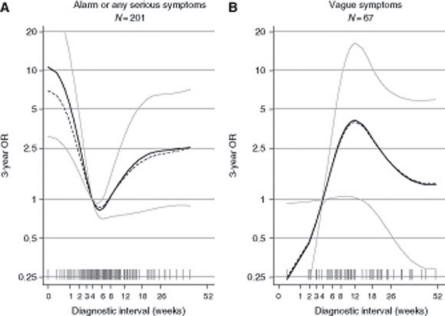
Methods: A total of 268 patients with CRC were included in a prospective, population-based study in a Danish county. The diagnostic interval was defined as the time from first presentation of symptoms until diagnosis. We analysed patients separately according to the general practitioner's interpretation of symptoms. Logistic regression was used to estimate 3-year mortality odds ratios as a function of the diagnostic interval using restricted cubic splines and adjusting for tumour site, comorbidity, age, and sex.
Results: In patients presenting with symptoms suggestive of cancer or any other serious illness, the risk of dying within 3 years decreased with diagnostic intervals up to 5 weeks and then increased (P=0.002). In patients presenting with vague symptoms, the association was reverse, although not statistically significant.
Conclusion: Detecting cancer in primary care is two sided: aimed at expediting ill patients while preventing healthy people from going to hospital. This likely explains the counterintuitive findings; but it does not explain the increasing mortality with longer diagnostic intervals. Thus, this study provides evidence for the hypothesis that the length of the diagnostic interval affects mortality in CRC patients.
Conflict of interest statement
The authors declare no conflict of interest. FO is the chairman of the Danish Cancer Society.
Figures
References
-
- Atkin WS, Edwards R, Kralj-Hans I, Wooldrage K, Hart AR, Northover JM, Parkin DM, Wardle J, Duffy SW, Cuzick J (2010) Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet 375: 1624–1633 - PubMed
-
- Auvinen A (1992) Social class and colon cancer survival in Finland. Cancer 70: 402–409 - PubMed
-
- Bako G, Hill GB, Ferenczi L, Hanson J (1988) Factors influencing the survival of patients with cancer of the colon or rectum. Chronic Dis Can 9: 101–104
-
- Barrett J, Jiwa M, Rose P, Hamilton W (2006) Pathways to the diagnosis of colorectal cancer: an observational study in three UK cities. Fam Pract 23: 15–19 - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40: 373–383 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
