

Impact of de-escalation therapy on clinical outcomes for intensive care unit-acquired pneumonia
- PMID: 21366903
- PMCID: PMC3219332
- DOI: 10.1186/cc10072
Impact of de-escalation therapy on clinical outcomes for intensive care unit-acquired pneumonia
Abstract
Introduction: De-escalation therapy is a strategy currently used for the management of nosocomial pneumonia. In this study, we evaluated clinical outcomes and risk factors related to de-escalation therapy in patients with intensive care unit (ICU)-acquired pneumonia.
Methods: This was a retrospective observational cohort study of ICU patients who developed pneumonia more than 48 hours after admission to the ICU at Samsung Medical Center from September 2004 to December 2007.
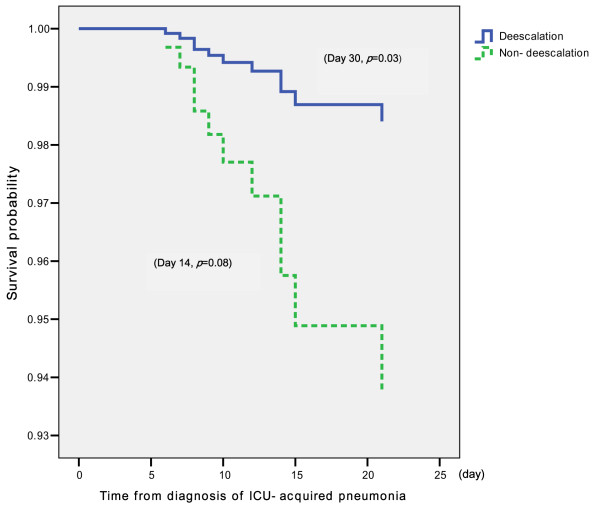
Results: The 137 patients comprised 44 (32.1%) who received de-escalation therapy and 93 in the non-de-escalation group. The de-escalation group showed a lower pneumonia-related mortality rate than the non-de-escalation group by day 14 (2.3% vs. 10.8%, respectively; P = 0.08) and by day 30 (2.3% vs. 14%, respectively; P = 0.03) after the diagnosis of pneumonia. The variables independently associated with ICU-acquired pneumonia-related mortality included the Acute Physiology and Chronic Health Evaluation II (APACHE II) score and the modified Clinical Pulmonary Infection Score (CPIS) after 5 days with pneumonia. The non-de-escalation group had significantly higher APACHE II score and modified CPIS after 5 days with ICU-acquired pneumonia compared to the de-escalation group. Among all patients, 20.4% (28 of 137) had negative cultures for pathogens, and 42.9% (12 of 28) received de-escalation therapy. The latter 12 patients received de-escalation therapy and survived 30 days after the diagnosis of pneumonia.
Conclusions: Patients in the de-escalation group showed a significantly lower mortality rate compared to patients in the non-de-escalation group. De-escalation therapy can be safely provided to patients with ICU-acquired pneumonia if they are clinically stable by day 5, even in those whose respiratory specimen cultures yield no specific pathogens.
Figures
References
-
- Rello J, Gallego M, Mariscal D, Soñora R, Valles J. The value of routine microbial investigation in ventilator-associated pneumonia. Am J Respir Crit Care Med. 1997;156:196–200. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
