

Patient safety, resident education and resident well-being following implementation of the 2003 ACGME duty hour rules
- PMID: 21369772
- PMCID: PMC3138977
- DOI: 10.1007/s11606-011-1657-1
Patient safety, resident education and resident well-being following implementation of the 2003 ACGME duty hour rules
Abstract
Context: The ACGME-released revisions to the 2003 duty hour standards.
Objective: To review the impact of the 2003 duty hour reform as it pertains to resident and patient outcomes.
Data sources: Medline (1989-May 2010), Embase (1989-June 2010), bibliographies, pertinent reviews, and meeting abstracts.
Study selection: We included studies examining the relationship between the pre- and post-2003 time periods and patient outcomes (mortality, complications, errors), resident education (standardized test scores, clinical experience), and well-being (as measured by the Maslach Burnout Inventory). We excluded non-US studies.
Data extraction: One rater used structured data collection forms to abstract data on study design, quality, and outcomes. We synthesized the literature qualitatively and included a meta-analysis of patient mortality.
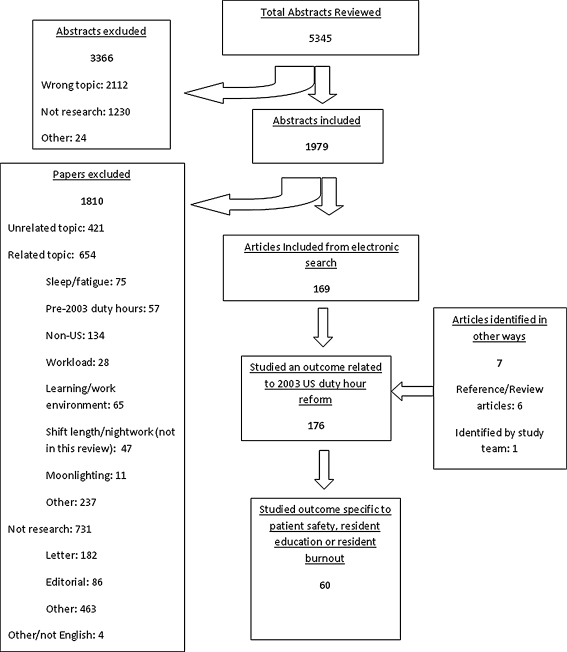
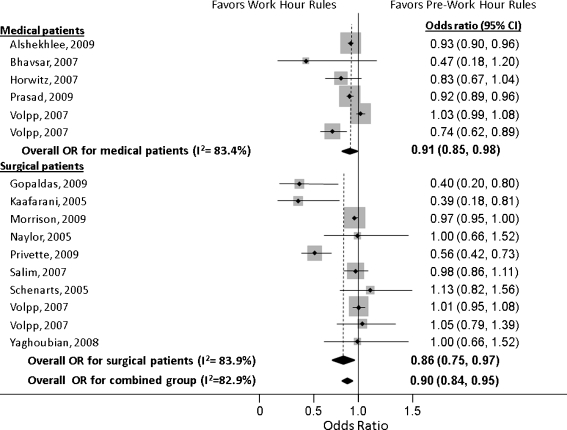
Results: Of 5,345 studies identified, 60 met eligibility criteria. Twenty-eight studies included an objective outcome related to patients; 10 assessed standardized resident examination scores; 26 assessed resident operative experience. Eight assessed resident burnout. Meta-analysis of the mortality studies revealed a significant improvement in mortality in the post-2003 time period with a pooled odds ratio (OR) of 0.9 (95% CI: 0.84, 0.95). These results were significant for medical (OR 0.91; 95% CI: 0.85, 0.98) and surgical patients (OR 0.86; 95% CI: 0.75, 0.97). However, significant heterogeneity was present (I(2) 83%). Patient complications were more nuanced. Some increased in frequency; others decreased. Outcomes for resident operative experience and standardized knowledge tests varied substantially across studies. Resident well-being improved in most studies.
Limitations: Most studies were observational. Not all studies of mortality provided enough information to be included in the meta-analysis. We used unadjusted odds ratios in the meta-analysis; statistical heterogeneity was substantial. Publication bias is possible.
Conclusions: Since 2003, patient mortality appears to have improved, although this could be due to secular trends. Resident well-being appears improved. Change in resident educational experience is less clear.
Figures
References
-
- Ulmer C, Wollman DM, Johns MME. Resident duty hours: Enhancing sleep, supervision, and safety. Washington DC: Institute of Medicine National Academies Press; 2008. - PubMed
-
- Nasca TJ, Day SH, Amis ES, Jr., The ADHTF: the new recommendations on duty hours from the ACGME task force. N Engl J Med: NEJMsb1005800. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
