

Should patients with abnormal liver function tests in primary care be tested for chronic viral hepatitis: cost minimisation analysis based on a comprehensively tested cohort
- PMID: 21371303
- PMCID: PMC3063222
- DOI: 10.1186/1471-2296-12-9
Should patients with abnormal liver function tests in primary care be tested for chronic viral hepatitis: cost minimisation analysis based on a comprehensively tested cohort
Abstract
Background: Liver function tests (LFTs) are ordered in large numbers in primary care, and the Birmingham and Lambeth Liver Evaluation Testing Strategies (BALLETS) study was set up to assess their usefulness in patients with no pre-existing or self-evident liver disease. All patients were tested for chronic viral hepatitis thereby providing an opportunity to compare various strategies for detection of this serious treatable disease.
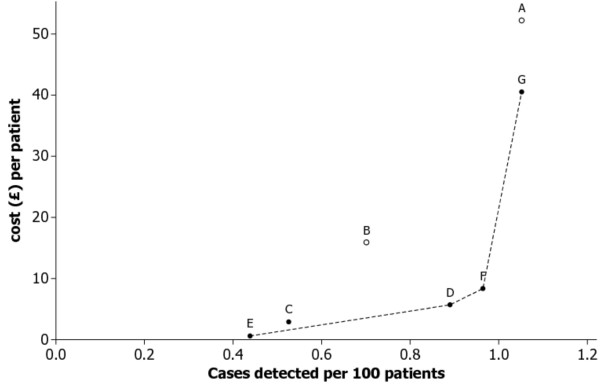
Methods: This study uses data from the BALLETS cohort to compare various testing strategies for viral hepatitis in patients who had received an abnormal LFT result. The aim was to inform a strategy for identification of patients with chronic viral hepatitis. We used a cost-minimisation analysis to define a base case and then calculated the incremental cost per case detected to inform a strategy that could guide testing for chronic viral hepatitis.
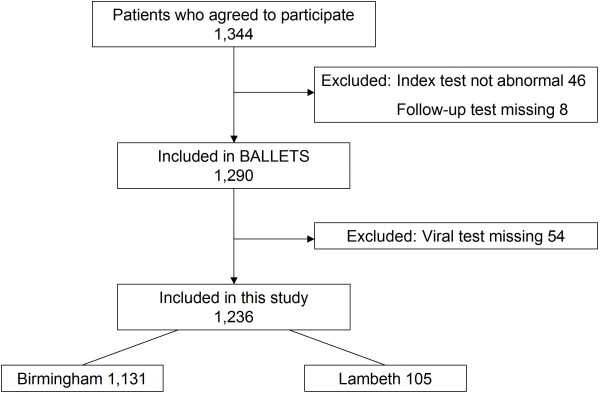
Results: Of the 1,236 study patients with an abnormal LFT, 13 had chronic viral hepatitis (nine hepatitis B and four hepatitis C). The strategy advocated by the current guidelines (repeating the LFT with a view to testing for specific disease if it remained abnormal) was less efficient (more expensive per case detected) than a simple policy of testing all patients for viral hepatitis without repeating LFTs. A more selective strategy of viral testing all patients for viral hepatitis if they were born in countries where viral hepatitis was prevalent provided high efficiency with little loss of sensitivity. A notably high alanine aminotransferase (ALT) level (greater than twice the upper limit of normal) on the initial ALT test had high predictive value, but was insensitive, missing half the cases of viral infection.
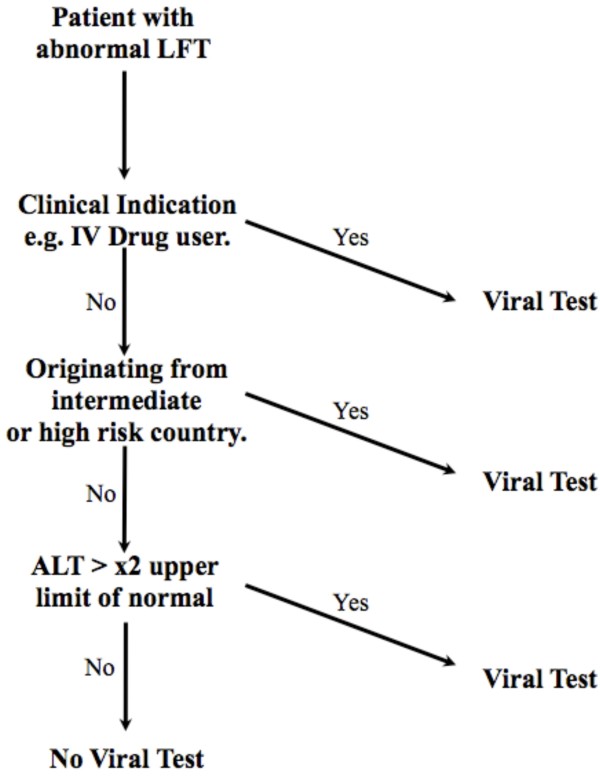
Conclusions: Based on this analysis and on widely accepted clinical principles, a "fast and frugal" heuristic was produced to guide general practitioners with respect to diagnosing cases of viral hepatitis in asymptomatic patients with abnormal LFTs. It recommends testing all patients where a clear clinical indication of infection is present (e.g. evidence of intravenous drug use), followed by testing all patients who originated from countries where viral hepatitis is prevalent, and finally testing those who have a notably raised ALT level (more than twice the upper limit of normal). Patients not picked up by this efficient algorithm had a risk of chronic viral hepatitis that is lower than the general population.
Figures
Similar articles
-
Birmingham and Lambeth Liver Evaluation Testing Strategies (BALLETS): a prospective cohort study.Health Technol Assess. 2013 Jul;17(28):i-xiv, 1-307. doi: 10.3310/hta17280. Health Technol Assess. 2013. PMID: 23834998 Free PMC article.
-
Clinical audit of quality of care among patients with viral hepatitis in primary care in a low endemic region.Fam Pract. 2024 Oct 8;41(5):693-701. doi: 10.1093/fampra/cmae019. Fam Pract. 2024. PMID: 38887051
-
Investigation of liver dysfunction: who should we test for hepatitis E?Eur J Gastroenterol Hepatol. 2017 Feb;29(2):215-220. doi: 10.1097/MEG.0000000000000781. Eur J Gastroenterol Hepatol. 2017. PMID: 27832041
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Treatment of chronic hepatitis B: case selection and duration of therapy.J Gastroenterol Hepatol. 2002 Apr;17(4):409-14. doi: 10.1046/j.1440-1746.2002.02767.x. J Gastroenterol Hepatol. 2002. PMID: 11982721 Review.
Cited by
-
Cost-effectiveness of the Three I's for HIV/TB and ART to prevent TB among people living with HIV.Int J Tuberc Lung Dis. 2014 Oct;18(10):1159-65. doi: 10.5588/ijtld.13.0571. Int J Tuberc Lung Dis. 2014. PMID: 25216828 Free PMC article.
-
Are the testing needs of key European populations affected by hepatitis B and hepatitis C being addressed? A scoping review of testing studies in Europe.Croat Med J. 2016 Oct 31;57(5):442-456. doi: 10.3325/cmj.2016.57.442. Croat Med J. 2016. PMID: 27815935 Free PMC article.
-
Ethnicity and the diagnosis gap in liver disease: a population-based study.Br J Gen Pract. 2014 Nov;64(628):e694-702. doi: 10.3399/bjgp14X682273. Br J Gen Pract. 2014. PMID: 25348993 Free PMC article.
-
Guidelines on the management of abnormal liver blood tests.Gut. 2018 Jan;67(1):6-19. doi: 10.1136/gutjnl-2017-314924. Epub 2017 Nov 9. Gut. 2018. PMID: 29122851 Free PMC article.
-
Case-finding for hepatitis C in primary care: a mixed-methods service evaluation.Br J Gen Pract. 2014 Feb;64(619):e67-74. doi: 10.3399/bjgp14X677112. Br J Gen Pract. 2014. PMID: 24567619 Free PMC article.
References
-
- Theal RM, Scott K. Evaluating asymptomatic patients with abnormal liver function test results. Am Fam Physician. 1996;53(6):2111–2119. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
