

New strategies in metastatic prostate cancer: targeting the androgen receptor signaling pathway
- PMID: 21372223
- PMCID: PMC3513706
- DOI: 10.1158/1078-0432.CCR-10-0567
New strategies in metastatic prostate cancer: targeting the androgen receptor signaling pathway
Abstract
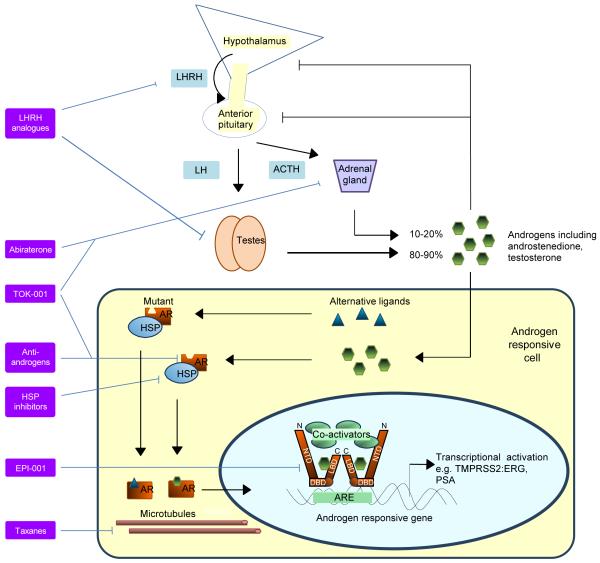
Recent data report that abiraterone acetate, a specific inhibitor of CYP17 that is key to androgen and estrogen synthesis, improves survival in metastatic castration-resistant prostate cancer (CRPC), confirming the continued dependency of CRPC on the androgen receptor (AR) signaling pathway. MDV3100 is a novel antagonist of AR that is also in phase III clinical trials. In addition, several other agents targeting the AR axis are undergoing evaluation in early clinical studies. CRPC patients progress on these therapies with an increasing prostate specific antigen (PSA), suggesting that repeated therapeutic interventions targeting the AR signaling axis could induce secondary responses and achieve prolonged clinical benefit for a subgroup of patients. These exciting results are good news for patients but introduce a number of treatment paradigm dilemmas for physicians. Clinical studies evaluating the ideal sequence of administration of these new agents, best timing for initiation, combination strategies, discontinuation beyond progression and after commencement of subsequent therapies, and coordination with other treatments have not been done. Predictive biomarkers could allow patient selection for a specific treatment, but in their absence, most physicians will rely on a trial of treatment with a preferred agent and substitute for an alternative therapy on objective progression. Current data suggest that the response rate to drugs targeting the AR ligand-binding domain decreases with each treatment, but we hypothesize that a significant proportion of CRPC remains dependent on the AR axis and, therefore, novel strategies for disrupting AR signaling merit evaluation.
Figures
References
-
- Huggins C, stevens RE, Jr, Hodges CV. Arch Surg. 1941;43:209.
-
- Ryan CJ, Smith MR, Fong L, Rosenberg JE, Kantoff P, Raynaud F, et al. Phase I Clinical Trial of the CYP17 Inhibitor Abiraterone Acetate Demonstrating Clinical Activity in Patients With Castration-Resistant Prostate Cancer Who Received Prior Ketoconazole Therapy. J Clin Oncol. 2010;28:1481–8. - PMC - PubMed
-
- Attard G, Reid AHM, Yap TA, Raynaud F, Dowsett M, Settatree S, et al. Phase I clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J Clin Oncol. 2008;26:4563–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
