

Might rare factors account for most of the mortality of preterm babies?
- PMID: 21372718
- PMCID: PMC3097041
- DOI: 10.1097/EDE.0b013e31821266c5
Might rare factors account for most of the mortality of preterm babies?
Abstract
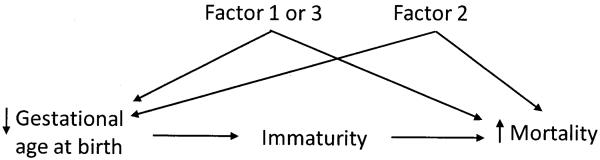
Background: Preterm delivery has a variety of causes, with each of these presumably carrying its own mortality risk. To the extent that they add to the risk of mortality, the various pathologic factors triggering preterm delivery will confound the causal contribution of gestational age to mortality, inflating the observed rates of gestational-age-specific mortality. We have previously estimated that about half of the mortality of US preterm singletons may be due to unmeasured pathologies that increase mortality risk and also cause preterm birth. In this paper, we examine the impact that rare factors may have, at least in theory, on preterm mortality.
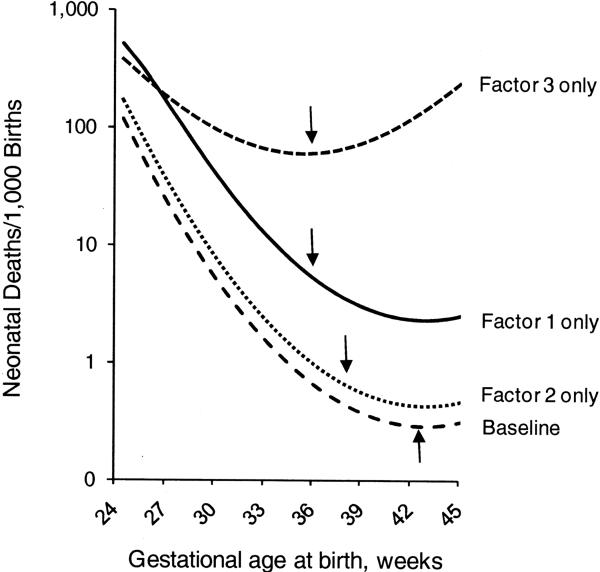
Methods: We constructed a simple model of gestational-age-specific mortality, in which we arbitrarily selected a function to represent the mortality due to immaturity alone ("baseline" risk). We then added "unmeasured" confounding factors that cause mortality and also cause preterm birth. This construct allowed us to calculate, in simple scenarios, the proportion of preterm mortality that could be caused by unmeasured confounding.
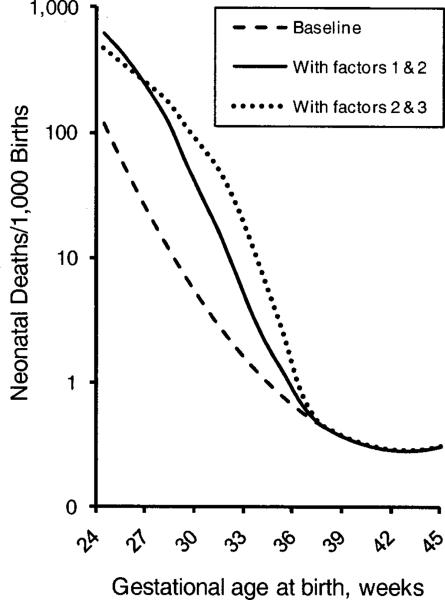
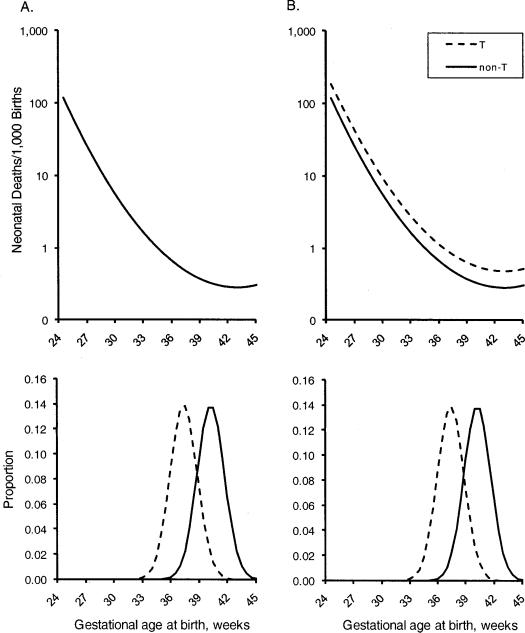
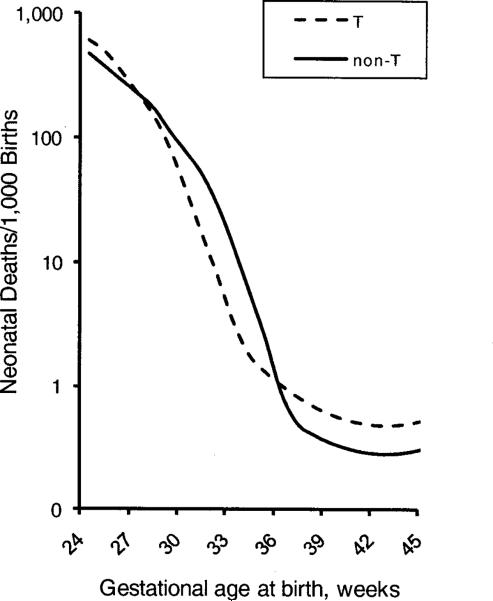
Results: We found that rare pathologies with moderate-to-strong effects can substantially contribute to preterm mortality. The presence of such rare factors can also produce an intersection of gestational-age-specific mortality curves when stratifying by known risk factors.
Conclusions: It is possible that a few relatively rare factors may account for a large fraction of preterm mortality. The search for such factors should be a primary focus of future research on preterm delivery.
Figures
Similar articles
-
Mortality risk among preterm babies: immaturity versus underlying pathology.Epidemiology. 2010 Jul;21(4):521-7. doi: 10.1097/EDE.0b013e3181debe5e. Epidemiology. 2010. PMID: 20407380 Free PMC article.
-
Outcomes in preterm infants.Public Health. 2014 May;128(5):399-403. doi: 10.1016/j.puhe.2014.03.010. Epub 2014 May 1. Public Health. 2014. PMID: 24794180 Review.
-
On the pitfalls of adjusting for gestational age at birth.Am J Epidemiol. 2011 Nov 1;174(9):1062-8. doi: 10.1093/aje/kwr230. Epub 2011 Sep 26. Am J Epidemiol. 2011. PMID: 21946386 Free PMC article.
-
The contribution of mild and moderate preterm birth to infant mortality. Fetal and Infant Health Study Group of the Canadian Perinatal Surveillance System.JAMA. 2000 Aug 16;284(7):843-9. doi: 10.1001/jama.284.7.843. JAMA. 2000. PMID: 10938173
-
Increase in preterm births in Brazil: review of population-based studies.Rev Saude Publica. 2008 Oct;42(5):957-64. doi: 10.1590/s0034-89102008000500023. Rev Saude Publica. 2008. PMID: 18833394 Review. English, Portuguese.
Cited by
-
Subtypes of preterm birth and the risk of postneonatal death.J Pediatr. 2013 Jan;162(1):28-34.e2. doi: 10.1016/j.jpeds.2012.06.051. Epub 2012 Aug 9. J Pediatr. 2013. PMID: 22878113 Free PMC article.
-
Causal inference in studies of preterm babies: a simulation study.BJOG. 2018 May;125(6):686-692. doi: 10.1111/1471-0528.14942. Epub 2017 Oct 30. BJOG. 2018. PMID: 28941068 Free PMC article.
-
Vanishing twins, selection in utero, and infant mortality in the United States.Evol Med Public Health. 2025 Jan 8;13(1):5-13. doi: 10.1093/emph/eoae035. eCollection 2025. Evol Med Public Health. 2025. PMID: 39845643 Free PMC article.
-
Re: "analyzing risks of adverse pregnancy outcomes".Am J Epidemiol. 2015 Feb 1;181(3):218. doi: 10.1093/aje/kwu463. Epub 2015 Jan 21. Am J Epidemiol. 2015. PMID: 25612573 Free PMC article. No abstract available.
-
Two denominators for one numerator: the example of neonatal mortality.Eur J Epidemiol. 2018 Jun;33(6):523-530. doi: 10.1007/s10654-018-0373-0. Epub 2018 Mar 7. Eur J Epidemiol. 2018. PMID: 29516296 Free PMC article.
References
-
- Romero R, Mazor M, Munoz H, et al. The preterm labor syndrome. Ann N Y Acad Sci. 1994;734:414–29. - PubMed
-
- Klebanoff MA, Schoendorf KC. Invited commentary: what's so bad about curves crossing anyway? Am J Epidemiol. 2004;160:211–2. discussion 215–6. - PubMed
-
- Gotsch F, Gotsch F, Romero R, et al. The preterm parturition syndrome and its implications for understanding the biology, risk assessment, diagnosis, treatment and prevention of preterm birth. J Matern Fetal Neonatal Med. 2009;22(Suppl 2):5–23. - PubMed
-
- Savitz DA. Invited commentary: disaggregating preterm birth to determine etiology. Am J Epidemiol. 2008;168:990–2. discussion 993–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
