

SMART syndrome: a late reversible complication after radiation therapy for brain tumours
- PMID: 21373901
- PMCID: PMC3101343
- DOI: 10.1007/s00415-010-5892-x
SMART syndrome: a late reversible complication after radiation therapy for brain tumours
Abstract
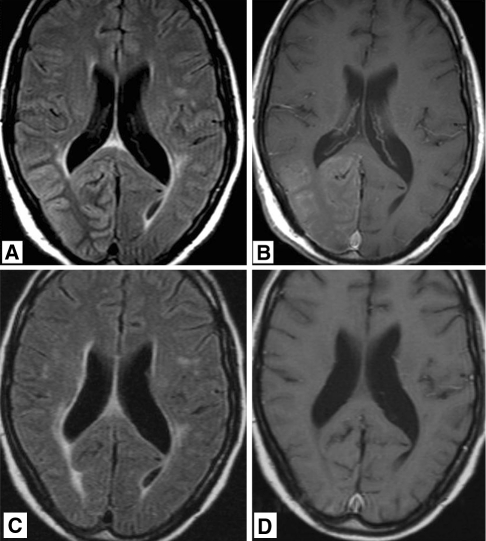
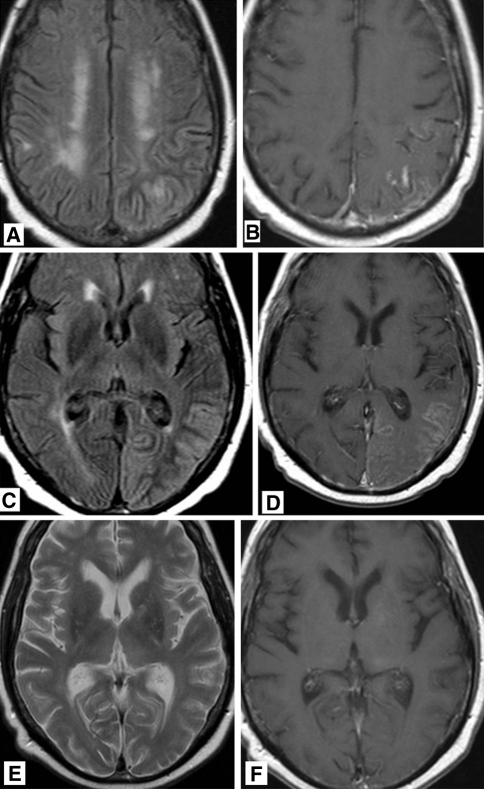
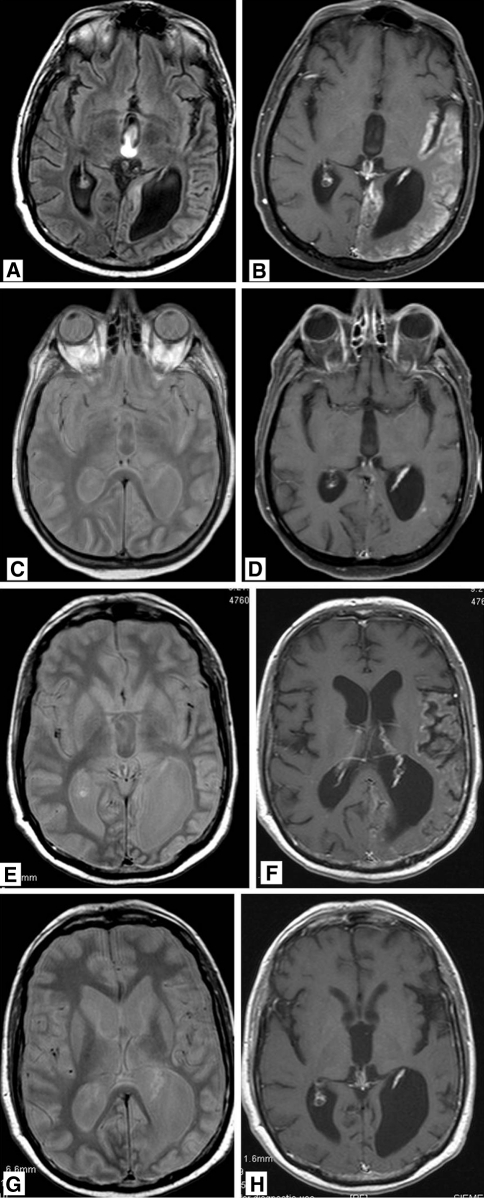
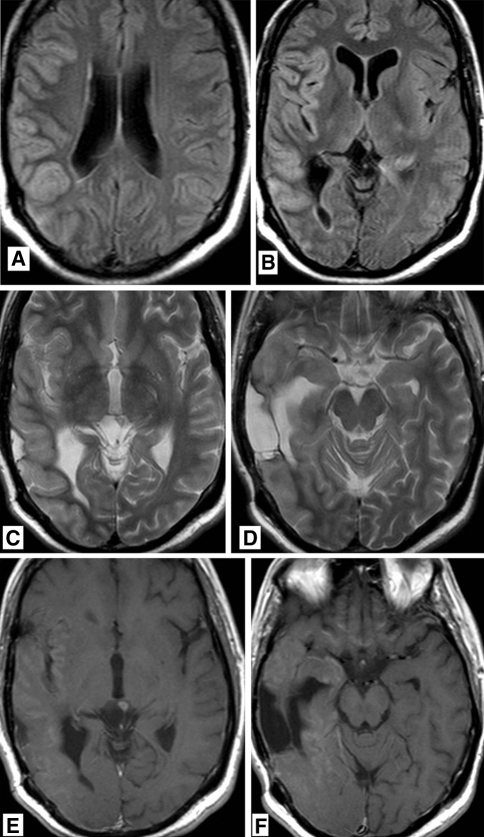
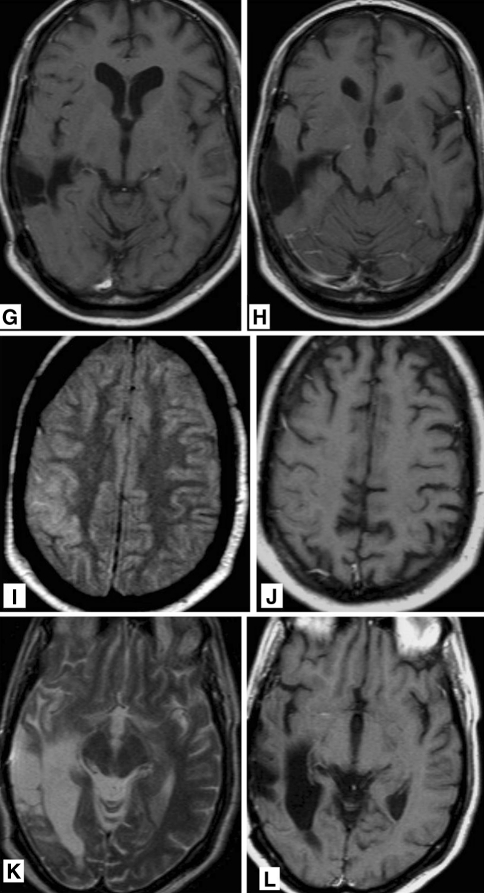
With intensified treatment leading to longer survival, complications of therapy for brain tumours are more frequently observed. Regarding radiation therapy, progressive and irreversible white matter disease with cognitive decline is most feared. We report on four patients with reversible clinical and radiological features occurring years after radiation for brain tumours, suggestive for the so called SMART syndrome (stroke-like migraine attacks after radiation therapy). All four patients (males, age 36-60 years) had been treated with focal brain radiation for a primary brain tumour or with whole-brain radiation therapy for brain metastases. Ranging from 2 to 10 years following radiation therapy patients presented with headache and focal neurological deficits, suggestive for tumour recurrence. Two patients also presented with focal seizures. MRI demonstrated typical cortical swelling and contrast enhancement, primarily in the parieto-occipital region. On follow-up both clinical and MRI features improved spontaneously. Three patients eventually proved to have tumour recurrence. The clinical and radiological picture of these patients is compatible with the SMART syndrome, a rare complication of radiation therapy which is probably under recognized in brain tumour patients. The pathophysiology of the SMART syndrome is poorly understood but bears similarities with the posterior reversible encephalopathy syndrome (PRES). These four cases underline that the SMART syndrome should be considered in patients formerly treated with radiation therapy for brain tumours, who present with new neurologic deficits. Before the diagnosis of SMART syndrome can be established other causes, such as local tumour recurrence, leptomeningeal disease or ischemic disease should be ruled out.
Figures
References
-
- Lachance DH, Black DF (2005) SMART: strokelike migraine attacks after radiation therapy. Neurology (Suppl 1) A220
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
