

Comparative effectiveness of pleural drainage procedures for the treatment of complicated pneumonia in childhood
- PMID: 21374798
- PMCID: PMC3112472
- DOI: 10.1002/jhm.872
Comparative effectiveness of pleural drainage procedures for the treatment of complicated pneumonia in childhood
Abstract
Objective: To determine the comparative effectiveness of common pleural drainage procedures for treatment of pneumonia complicated by parapneumonic effusion (ie, complicated pneumonia).
Design: Multicenter retrospective cohort study.
Setting: Forty children's hospitals contributing data to the Pediatric Health Information System.
Participants: Children with complicated pneumonia requiring pleural drainage.
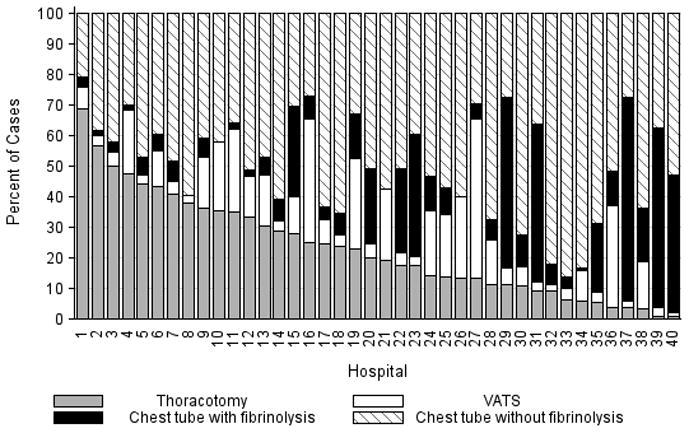
Main exposures: Initial drainage procedures were categorized as chest tube without fibrinolysis, chest tube with fibrinolysis, video-assisted thoracoscopic surgery (VATS), and thoracotomy.
Main outcome measures: Length of stay (LOS), additional drainage procedures, readmission within 14 days of discharge, and hospital costs.
Results: Initial procedures among 3500 patients included chest tube without fibrinolysis (n = 1762), chest tube with fibrinolysis (n = 623), VATS (n = 408), and thoracotomy (n = 797). Median age was 4.1 years. Overall, 716 (20.5%) patients received an additional drainage procedure (range, 6.8-44.8% across individual hospitals). The median LOS was 10 days (range, 7-14 days across individual hospitals). The median readmission rate was 3.8% (range, 0.8%-33.3%). In multivariable analysis, differences in LOS by initial procedure type were not significant. Patients undergoing initial chest tube placement with or without fibrinolysis were more likely to require additional drainage procedures. However, initial chest tube without fibrinolysis was the least costly strategy.
Conclusion: There is variability in the treatment and outcomes of children with complicated pneumonia. Outcomes were similar in patients undergoing initial chest tube placement with or without fibrinolysis. Those undergoing VATS received fewer additional drainage procedures but had no differences in LOS compared with other strategies.
Copyright © 2011 Society of Hospital Medicine.
Conflict of interest statement
Figures
References
-
- Chonmaitree T, Powell KR. Parapneumonic pleural effusion and empyema in children. Review of a 19-year experience, 1962–1980. Clin Pediatr (Phila) 1983;22:414–9. - PubMed
-
- Shah SS, DiCristina CM, Bell LM, Ten Have T, Metlay JP. Primary early thoracoscopy and reduction in length of hospital stay and additional procedures among children with complicated pneumonia: results of a multicenter retrospective cohort study. Arch Pediatr Adolesc Med. 2008;162:675–81. - PubMed
-
- Li ST, Tancredi DJ. Empyema hospitalizations increased in US children despite pneumococcal conjugate vaccine. Pediatrics. 2010;125:26–33. - PubMed
-
- Byington CL, Korgenski K, Daly J, Ampofo K, Pavia A, Mason EO. Impact of the pneumococcal conjugate vaccine on pneumococcal parapneumonic empyema. Pediatr Infect Dis J. 2006;25:250–4. - PubMed
-
- Hendrickson DJ, Blumberg DA, Joad JP, Jhawar S, McDonald RJ. Five-fold increase in pediatric parapneumonic empyema since introduction of pneumococcal conjugate vaccine. Pediatric Infectious Disease Journal. 2008;27:1030–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
