

Low-dose radiation exposure and atherosclerosis in ApoE⁻/⁻ mice
- PMID: 21375359
- PMCID: PMC3998759
- DOI: 10.1667/RR2176.1
Low-dose radiation exposure and atherosclerosis in ApoE⁻/⁻ mice
Abstract
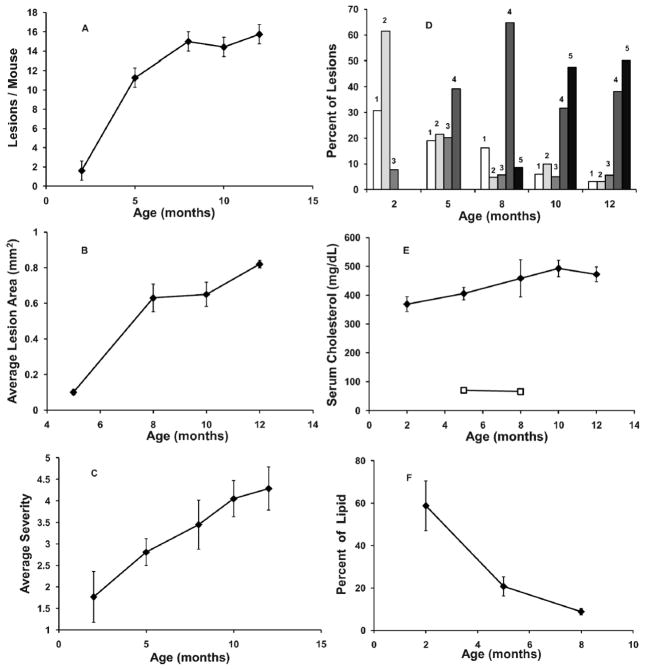
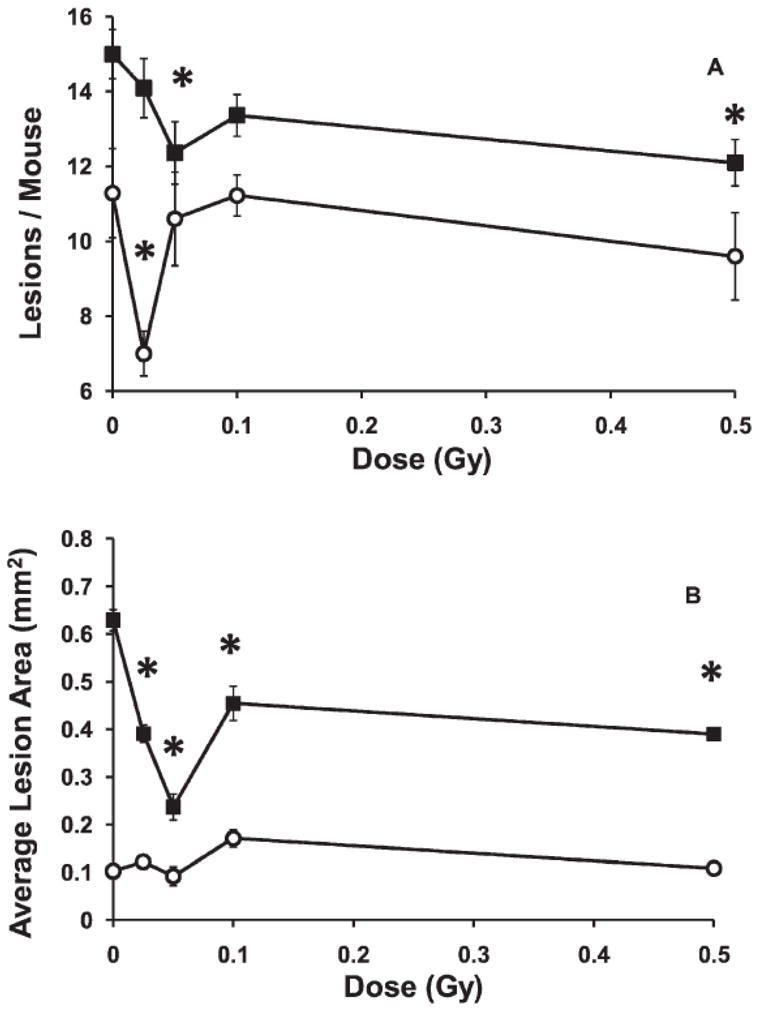
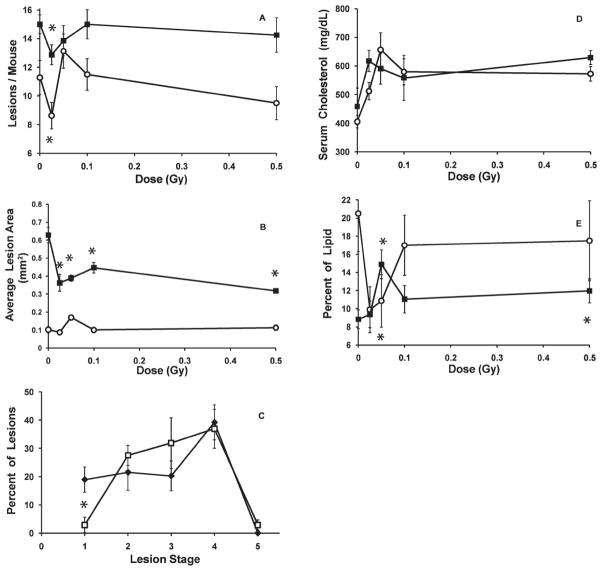
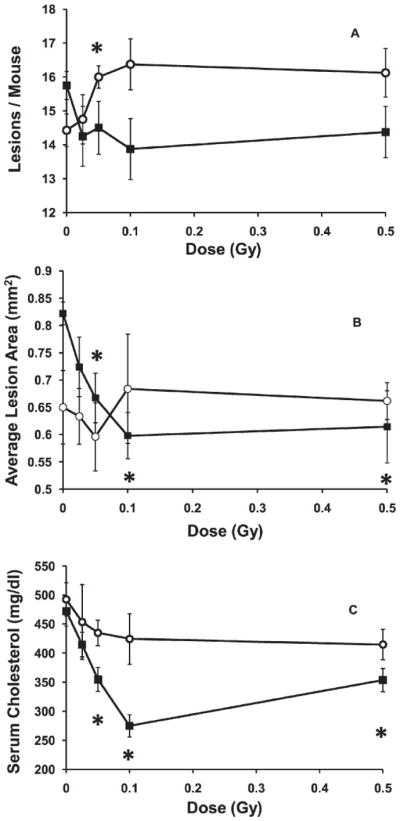
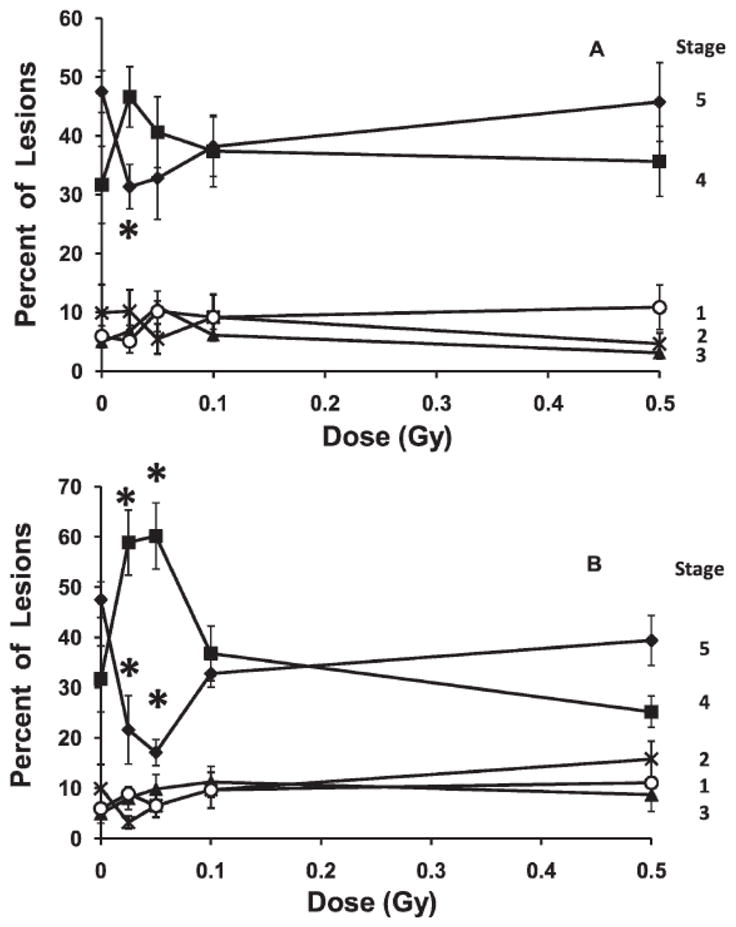
The hypothesis that single low-dose exposures (0.025-0.5 Gy) to low-LET radiation given at either high (about 150 mGy/min) or low (1 mGy/min) dose rate would promote aortic atherosclerosis was tested in female C57BL/6J mice genetically predisposed to this disease (ApoE⁻/⁻). Mice were exposed either at an early stage of disease (2 months of age) and examined 3 or 6 months later or at a late stage of disease (8 months of age) and examined 2 or 4 months later. Changes in aortic lesion frequency, size and severity as well as total serum cholesterol levels and the uptake of lesion lipids by lesion-associated macrophages were assessed. Statistically significant changes in each of these measures were observed, depending on dose, dose rate and disease stage. In all cases, the results were distinctly non-linear with dose, with maximum effects tending to occur at 25 or 50 mGy. In general, low doses given at low dose rate during either early- or late-stage disease were protective, slowing the progression of the disease by one or more of these measures. Most effects appeared and persisted for months after the single exposures, but some were ultimately transitory. In contrast to exposure at low dose rate, high-dose-rate exposure during early-stage disease produced both protective and detrimental effects, suggesting that low doses may influence this disease by more than one mechanism and that dose rate is an important parameter. These results contrast with the known, generally detrimental effects of high doses on the progression of this disease in the same mice and in humans, suggesting that a linear extrapolation of the known increased risk from high doses to low doses is not appropriate.
Figures
References
-
- Shimizu Y, Pierce DA, Preston DL, Mabuchi K. Studies of the mortality of atomic bomb survivors. Report 12, part II. Noncancer mortality: 1950–1990. Radiat Res. 1999;152:374–389. - PubMed
-
- Yamada M, Wong FL, Fujiwara S, Akahoshi M, Suzuki G. Noncancer disease incidence in atomic bomb survivors, 1958–1998. Radiat Res. 2004;161:622–632. - PubMed
-
- Preston DL, Shimizu Y, Pierce DA, Suyama A, Mabuchi K. Studies of mortality of atomic bomb survivors. Report 13: Solid cancer and noncancer disease mortality: 1950–1997. Radiat Res. 2003;160:381–407. - PubMed
-
- Yamada M, Naito K, Kasagi F, Masunari N, Suzuki G. Prevalence of atherosclerosis in relation to atomic bomb radiation exposure: an RERF Adult Health Study. Int J Radiat Biol. 2005;81:821–826. - PubMed
-
- Carr ZA, Land CE, Kleinerman RA, Weinstock RW, Stovall M, Griem ML, Mabuchi K. Coronary heart disease after radiotherapy for peptic ulcer disease. Int J Radiat Oncol Biol Phys. 2005;61:842–850. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
