

Neurologic bases for comorbidity of balance disorders, anxiety disorders and migraine: neurotherapeutic implications
- PMID: 21375443
- PMCID: PMC3107725
- DOI: 10.1586/ern.11.19
Neurologic bases for comorbidity of balance disorders, anxiety disorders and migraine: neurotherapeutic implications
Abstract
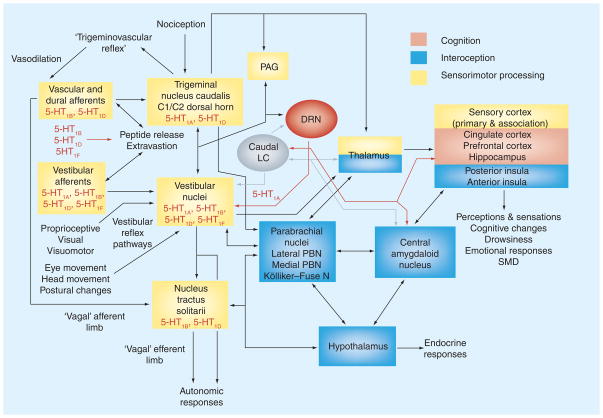
The comorbidity among balance disorders, anxiety disorders and migraine has been studied extensively from clinical and basic research perspectives. From a neurological perspective, the comorbid symptoms are viewed as the product of sensorimotor, interoceptive and cognitive adaptations that are produced by afferent interoceptive information processing, a vestibulo-parabrachial nucleus network, a cerebral cortical network (including the insula, orbitofrontal cortex, prefrontal cortex and anterior cingulate cortex), a raphe nuclear-vestibular network, a coeruleo-vestibular network and a raphe-locus coeruleus loop. As these pathways overlap extensively with pathways implicated in the generation, perception and regulation of emotions and affective states, the comorbid disorders and effective treatment modalities can be viewed within the contexts of neurological and psychopharmacological sites of action of current therapies.
Figures
References
-
- Furman JM, Jacob RG. A clinical taxonomy of dizziness and anxiety in the otoneurologic setting. J Anxiety Disord. 2001;15:9–26. - PubMed
-
- Jacob RG, Furman JM, Balaban CD. Psychiatric aspects of vestibular disorders. In: Baloh RW, Halmagyi GM, editors. Handbook of Neurotology/Vestibular System. Oxford University Press; Oxford, UK: 1996. pp. 509–528.
-
- Staab JP. Chronic dizziness: the interface between psychiatry and neuro-otology. Curr Opin Neurol. 2006;19(1):41–48. - PubMed
-
- Staab JP, Ruckenstein MJ. Chronic dizziness and anxiety: effect of course of illness on treatment outcome. Arch Otolaryngol Head Neck Surg. 2005;131(8):675–679. - PubMed
-
- Staab JP, Ruckenstein MJ. Expanding the differential diagnosis of chronic dizziness. Arch Otolaryngol Head Neck Surg. 2007;133:170–176. - PubMed
Websites
-
- Facts for Physicians on mild TBI. 2010 www.cdc.gov/concussion/headsup/pdf/Facts_for_Physicians_booklet-a.pdf.
-
- Hoffer ME, Balaban CD. Neurotologic consequences of blast injury. IBIA NeuroTrauma Letter. 2010 www.internationalbrain.org/?q=node/151.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials