

Accelerated progression from islet autoimmunity to diabetes is causing the escalating incidence of type 1 diabetes in young children
- PMID: 21376535
- PMCID: PMC3110538
- DOI: 10.1016/j.jaut.2011.02.004
Accelerated progression from islet autoimmunity to diabetes is causing the escalating incidence of type 1 diabetes in young children
Abstract
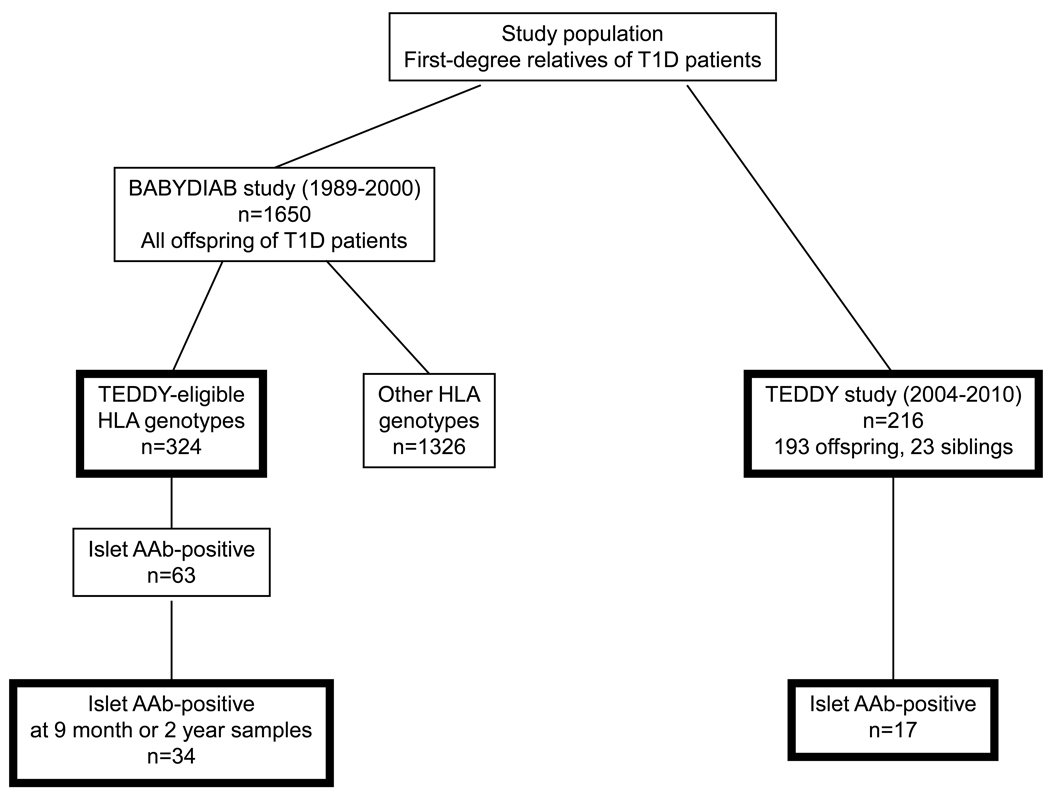
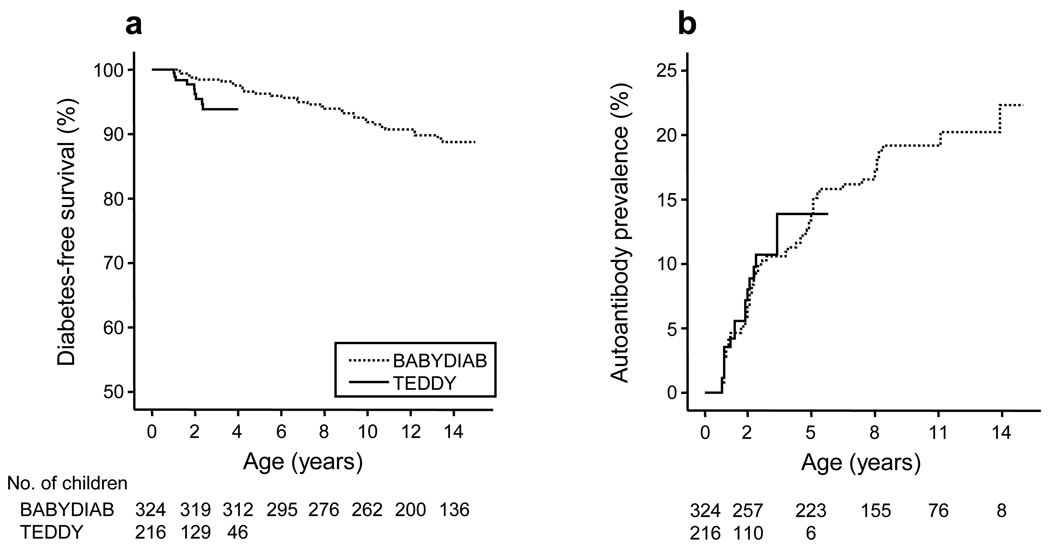
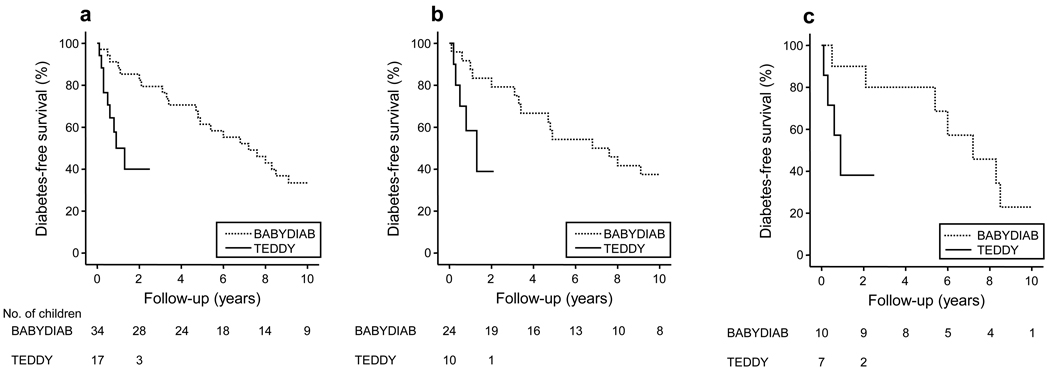
The incidence of type 1 diabetes is rising worldwide, particularly in young children. Since type 1 diabetes is preceded by autoimmunity to islet antigens, there must be a consequent increase in the incidence of islet autoimmunity in young children or a more rapid rate of progression to diabetes once islet autoimmunity initiates. This study was to determine whether the incidence of islet autoimmunity or the rate of progression from autoimmunity to diabetes onset has changed over a 20-year period in children genetically predisposed to type 1 diabetes. Between 1989 and 2010, children who were first-degree relatives of patients with type 1 diabetes and who were born in Germany were prospectively followed from birth without intervention. A total of 324 children (BABYDIAB study) born between 1989 and 2000 and 216 children (TEDDY study) born between 2004 and 2010 with matched HLA genotypes were recruited before age 3 months and included for analysis. Children were followed for the development of autoantibodies to insulin, GAD, and IA-2, and for progression to diabetes. The cumulative frequency of diabetes by age 4 years was 2.5% (95% CI 0.8-4.2%) in BABYDIAB children and 6.2% (95% CI 2.3-10.1%) in TEDDY children (p = 0.03). The cumulative frequency of islet autoantibodies by age 4 years was similar in the children from both studies (11.3% vs 13.9%). Progression to diabetes from the development of islet autoantibodies was markedly increased in autoantibody-positive children from the more recently recruited TEDDY cohort (50% progression within 85.2 months for BABYDIAB children vs 9.6 months for TEDDY children; p = 0.009), also if children were further selected on the basis of high-risk HLA genotypes or the development of autoantibodies to multiple islet antigens (p = 0.01). The findings suggest that recent increasing incidence of type 1 diabetes in young children could be due to weakening of mechanisms that normally regulate autoimmune destruction of islet beta cells.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
The recent rise in the frequency of type 1 diabetes: who pulled the trigger?J Autoimmun. 2011 Aug;37(1):1-2. doi: 10.1016/j.jaut.2011.04.001. J Autoimmun. 2011. PMID: 21641185 Free PMC article. No abstract available.
References
-
- Patterson CC, Dahlquist GG, Gyurus E, Green A, Soltesz G. Incidence trends for childhood type 1 diabetes in Europe during 1989–2003 and predicted new cases 2005–20: a multicentre prospective registration study. Lancet. 2009;373:2027–2033. - PubMed
-
- Karvonen M, Pitkaniemi J, Tuomilehto J. The onset age of type 1 diabetes in Finnish children has become younger. The Finnish Childhood Diabetes Registry Group. Diabetes Care. 1999;22:1066–1070. - PubMed
-
- Harjutsalo V, Sjoberg L, Tuomilehto J. Time trends in the incidence of type 1 diabetes in Finnish children: a cohort study. Lancet. 2008;371:1777–1782. - PubMed
-
- Dabelea D, Bell RA, D'Agostino RB, Jr, Imperatore G, Johansen JM, Linder B, et al. Incidence of diabetes in youth in the United States. JAMA. 2007;297:2716–2724. - PubMed
-
- Atkinson MA, Eisenbarth GS. Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet. 2001;358:221–229. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
