

Increased left ventricular mass and decreased left ventricular systolic function have independent pathways to ventricular arrhythmogenesis in coronary artery disease
- PMID: 21376836
- PMCID: PMC3123721
- DOI: 10.1016/j.hrthm.2011.02.037
Increased left ventricular mass and decreased left ventricular systolic function have independent pathways to ventricular arrhythmogenesis in coronary artery disease
Abstract
Background: Following myocardial infarction, individual patients can have wide variations in the extent of left ventricular systolic dysfunction (LVSD) and increased left ventricular (LV) mass. Both affect the risk for sudden cardiac death, but only LV ejection fraction is used for risk prediction.
Objective: The purpose of this study was to evaluate the independent as well as the additive contributions of increased LV mass and decreased LV ejection fraction to sudden cardiac death in the general population.
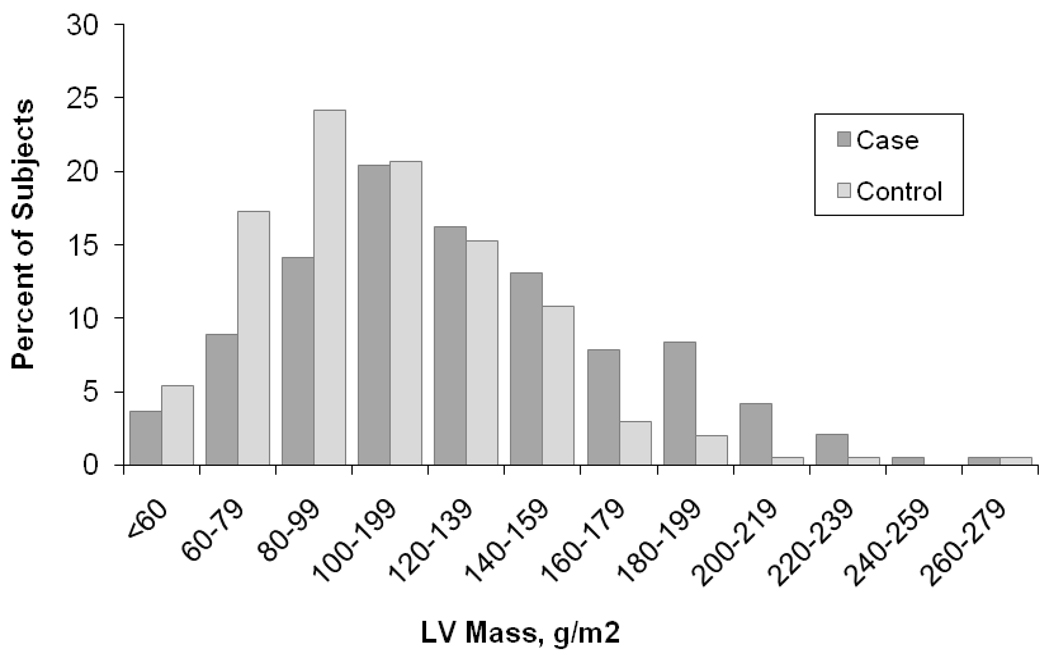
Methods: In the ongoing Oregon Sudden Unexpected Death Study, we studied consecutive SCD cases (n = 191) and coronary artery disease controls (n = 203) from the Portland, Oregon, metropolitan area (population approximately 1,000,000; 2002-2008). Comparisons of echocardiographic LV mass obtained prior and unrelated to sudden cardiac death (SCD) were conducted, and a logistic regression model was used to evaluate the relationship between SCD, severe LVSD, LV mass, and other relevant clinical variables.
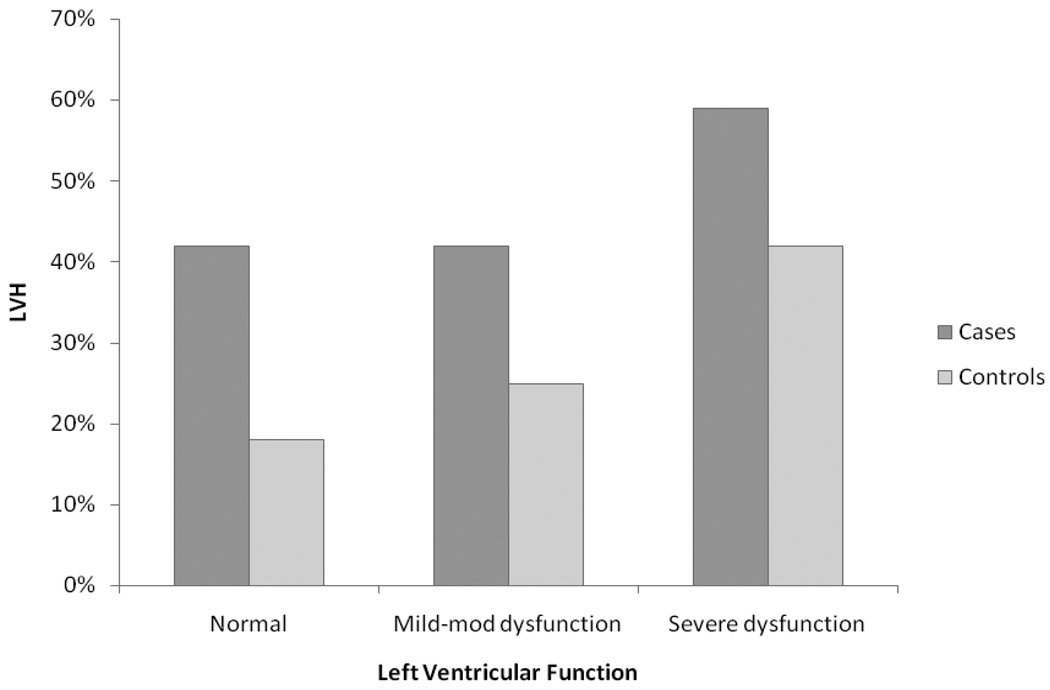
Results: In a multivariate model, both severe LVSD and left ventricular hypertrophy (LVH) were associated with increased SCD risk (odds ratio [OR] 1.9, 95% confidence interval [CI] 1.1-3.2 for severe LVSD; OR 1.8, 95% CI 1.1-2.9 for LVH). In patients with coexisting severe LVSD and LVH, risk of SCD was additive (OR 3.5, 95% CI 1.7-7.2). In the same model, increased age, atrial fibrillation/flutter, elevated creatinine, and diabetes independently increased risk, and use of angiotensin receptor blockers attenuated risk.
Conclusion: Reduced LV ejection fraction and increased LV mass had independent and additive effects on risk of sudden death. Despite the significant overlap between the two conditions, these findings point toward the existence of independent mechanistic pathways for ventricular arrhythmias that occur due to LVSD and LVH.
Copyright © 2011 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

Comment in
-
Sudden cardiac death won't go away: what are we to do?Heart Rhythm. 2011 Aug;8(8):1183-4. doi: 10.1016/j.hrthm.2011.04.016. Epub 2011 Apr 15. Heart Rhythm. 2011. PMID: 21699829 No abstract available.
References
-
- Buxton AE. Identifying the high risk patient with coronary artery disease--is ejection fraction all you need? J Cardiovasc Electrophysiol. 2005;16 Suppl 1:S25–S27. - PubMed
-
- de Vreede-Swagemakers JJ, Gorgels AP, Dubois-Arbouw WI, et al. Out-of-hospital cardiac arrest in the 1990's: a population-based study in the Maastricht area on incidence, characteristics and survival. J Am Coll Cardiol. 1997;30:1500–1505. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
