

A randomized controlled study of peanut oral immunotherapy: clinical desensitization and modulation of the allergic response
- PMID: 21377034
- PMCID: PMC3060783
- DOI: 10.1016/j.jaci.2010.12.1111
A randomized controlled study of peanut oral immunotherapy: clinical desensitization and modulation of the allergic response
Abstract
Background: Open-label oral immunotherapy (OIT) protocols have been used to treat small numbers of patients with peanut allergy. Peanut OIT has not been evaluated in double-blind, placebo-controlled trials.
Objective: To investigate the safety and effectiveness of OIT for peanut allergy in a double-blind, placebo-controlled study.
Methods: In this multicenter study, children ages 1 to 16 years with peanut allergy received OIT with peanut flour or placebo. Initial escalation, build-up, and maintenance phases were followed by an oral food challenge (OFC) at approximately 1 year. Titrated skin prick tests (SPTs) and laboratory studies were performed at regular intervals.
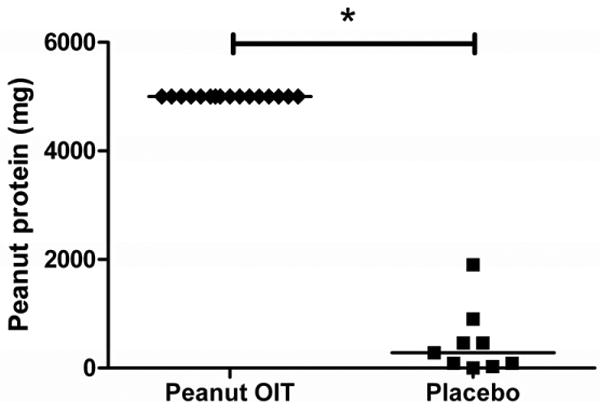
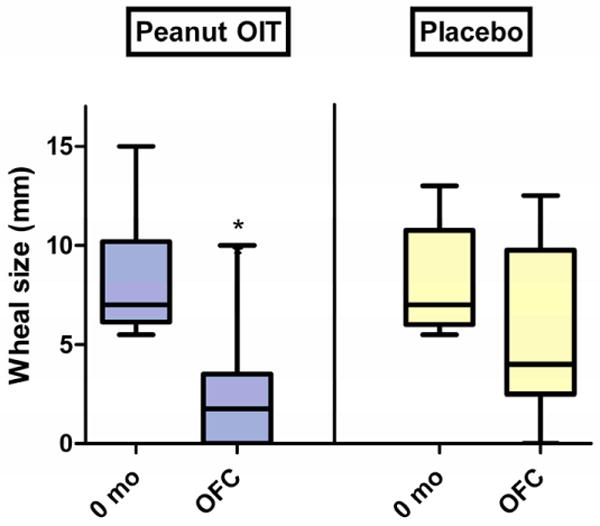
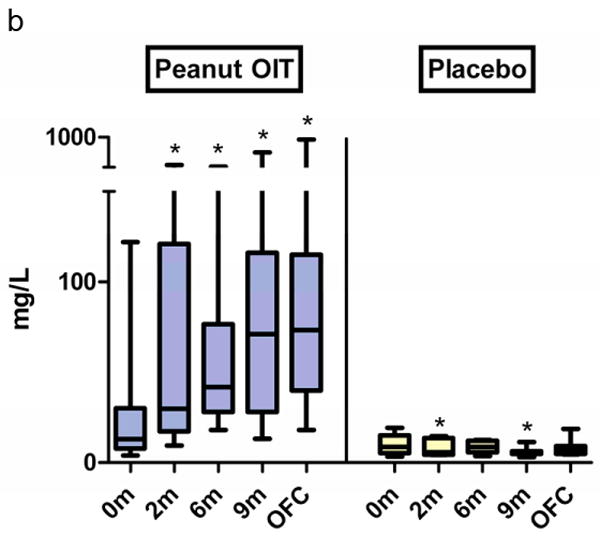
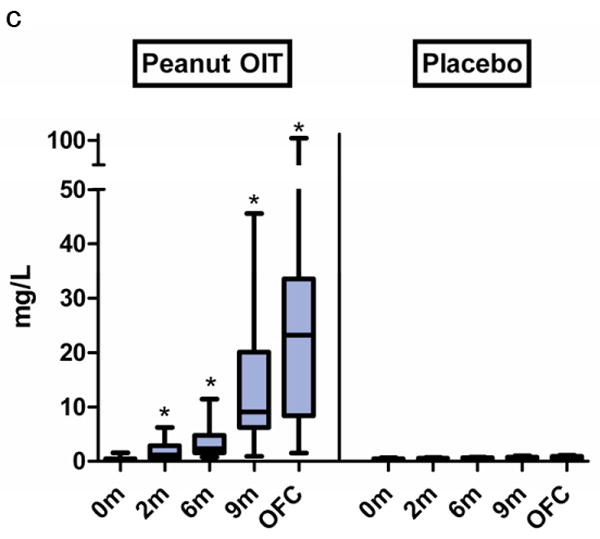
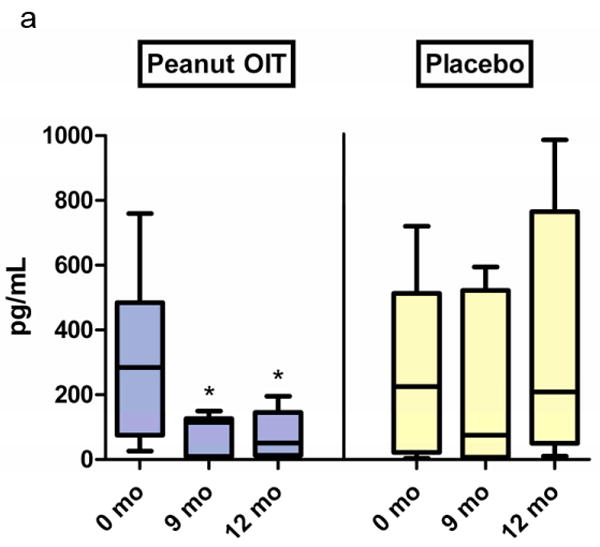
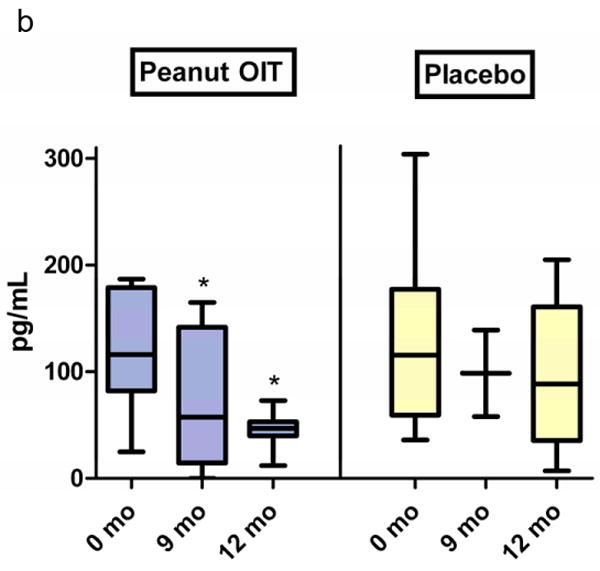
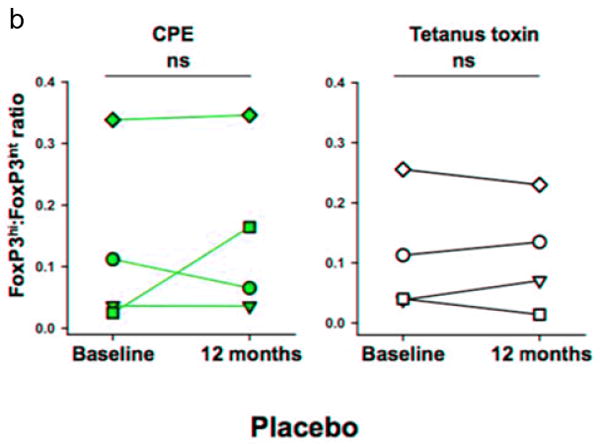
Results: Twenty-eight subjects were enrolled in the study. Three peanut OIT subjects withdrew early in the study because of allergic side effects. During the double-blind, placebo-controlled food challenge, all remaining peanut OIT subjects (n = 16) ingested the maximum cumulative dose of 5000 mg (approximately 20 peanuts), whereas placebo subjects (n = 9) ingested a median cumulative dose of 280 mg (range, 0-1900 mg; P < .001). In contrast with the placebo group, the peanut OIT group showed reductions in SPT size (P < .001), IL-5 (P = .01), and IL-13 (P = .02) and increases in peanut-specific IgG(4) (P < .001). Peanut OIT subjects had initial increases in peanut-specific IgE (P < .01) but did not show significant change from baseline by the time of OFC. The ratio of forkhead box protein 3 (FoxP3)(hi): FoxP3(intermediate) CD4+ CD25+ T cells increased at the time of OFC (P = .04) in peanut OIT subjects.
Conclusion: These results conclusively demonstrate that peanut OIT induces desensitization and concurrent immune modulation. The current study continues and is evaluating the hypothesis that peanut OIT causes long-term immune tolerance.
Copyright © 2011 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures


References
-
- Branum AM, Lukacs SL. Food allergy among U.S. children: trends in prevalence and hospitalizations. NCHS Data Brief. 2008 Oct;(10):1–8. - PubMed
-
- Sicherer SH, Munoz-Furlong A, Sampson HA. Prevalence of peanut and tree nut allergy in the United States determined by means of a random digit dial telephone survey: a 5-year follow-up study. J Allergy Clin Immunol. 2003 Dec;112(6):1203–7. - PubMed
-
- Bock SA, Munoz-Furlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J Allergy Clin Immunol. 2001 Jan;107(1):191–3. - PubMed
-
- Bock SA, Munoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001-2006. J Allergy Clin Immunol. 2007 Apr;119(4):1016–8. - PubMed
-
- Fleischer DM. The natural history of peanut and tree nut allergy. Curr Allergy Asthma Rep. 2007 Jun;7(3):175–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
