

Decreased response to inhaled steroids in overweight and obese asthmatic children
- PMID: 21377042
- PMCID: PMC3056233
- DOI: 10.1016/j.jaci.2010.12.010
Decreased response to inhaled steroids in overweight and obese asthmatic children
Abstract
Background: The mechanisms and consequences of the observed association between obesity and childhood asthma are unclear.
Objectives: We sought to determine the effect of obesity on treatment responses to inhaled corticosteroids in asthmatic children.
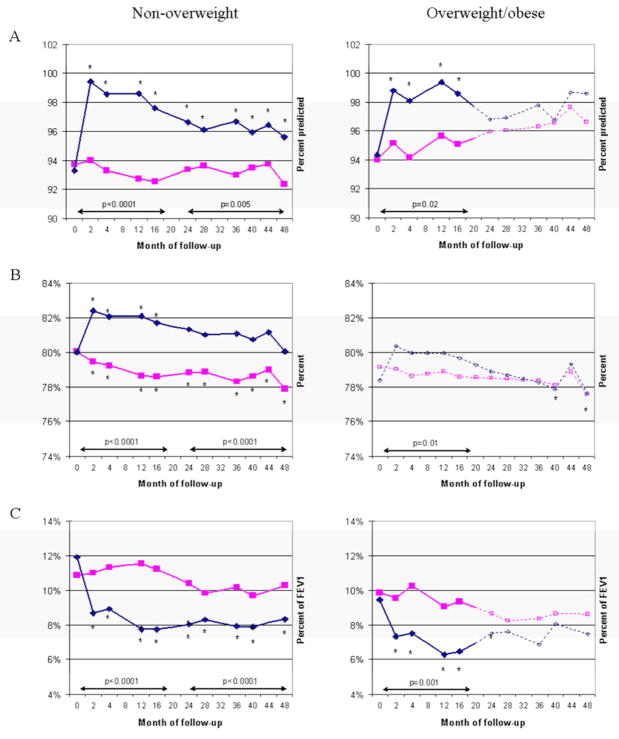
Methods: We performed a post hoc analysis to evaluate the interaction between body mass index (BMI) and treatment with inhaled budesonide on lung function in the Childhood Asthma Management Program trial. Participants were then stratified into overweight/obese and nonoverweight groups, and their response to inhaled budesonide was analyzed longitudinally over the 4 years of the trial.
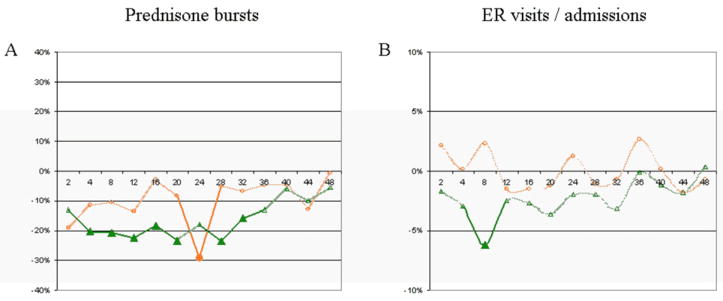
Results: There was a significant interaction between BMI and budesonide for prebronchodilator FEV(1)/forced vital capacity (FVC) ratio (P = .0007) and bronchodilator response (BDR; P = .049) and a nonsignificant trend for an interaction between BMI and budesonide on prebronchodilator FEV(1) (P = .15). Nonoverweight children showed significant improvement with inhaled budesonide in lung function (FEV(1), FEV(1)/FVC ratio, and BDR) during the early (years 1-2) and late (years 3-4) stages of the trial. Overweight/obese children had improved FEV(1) and BDR during the early but not the late stage of the trial and showed no improvement in FEV(1)/FVC ratio. When comparing time points at which both groups showed a significant response, the degree of improvement among nonoverweight children was significantly greater than in overweight/obese children at most visits. Nonoverweight children had a 44% reduction in the risk of emergency department visits or hospitalizations throughout the trial (P = .001); there was no reduction in risk among overweight/obese children (P = .97).
Conclusions: Compared with children of normal weight, overweight/obese children in the Childhood Asthma Management Program showed a decreased response to inhaled budesonide on measures of lung function and emergency department visits/hospitalizations for asthma.
Copyright © 2011 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Kotseva K, Wood D, De Backer G, De Bacquer D, Pyorala K, Keil U. Cardiovascular prevention guidelines in daily practice: a comparison of EUROASPIRE I, II, and III surveys in eight European countries. Lancet. 2009 Mar 14;373(9667):929–40. - PubMed
-
- Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1(1):11–25. - PubMed
-
- Akinbami L. The state of childhood asthma, United States, 1980–2005. Adv Data. 2006 Dec;12(381):1–24. - PubMed
-
- Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among US children and adolescents, 1999–2000. JAMA. 2002 Oct 9;288(14):1728–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01-HR-16046/HR/NHLBI NIH HHS/United States
- N01-HR-16051/HR/NHLBI NIH HHS/United States
- M01 RR002719/RR/NCRR NIH HHS/United States
- N01-HR-16044/HR/NHLBI NIH HHS/United States
- N01-HR-16048/HR/NHLBI NIH HHS/United States
- M01 RR000036/RR/NCRR NIH HHS/United States
- N01 HR016044/HL/NHLBI NIH HHS/United States
- N01-HR-16045/HR/NHLBI NIH HHS/United States
- N01-HR-16052/HR/NHLBI NIH HHS/United States
- M01RR02719-14/RR/NCRR NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- N01-HR-16050/HR/NHLBI NIH HHS/United States
- N01-HR-16047/HR/NHLBI NIH HHS/United States
- N01-HR-16049/HR/NHLBI NIH HHS/United States
- RR00036/RR/NCRR NIH HHS/United States
- M01RR00051/RR/NCRR NIH HHS/United States
- M01RR0099718-24/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
