

Understanding gastrointestinal distress: a framework for clinical practice
- PMID: 21378758
- PMCID: PMC4275100
- DOI: 10.1038/ajg.2010.383
Understanding gastrointestinal distress: a framework for clinical practice
Abstract
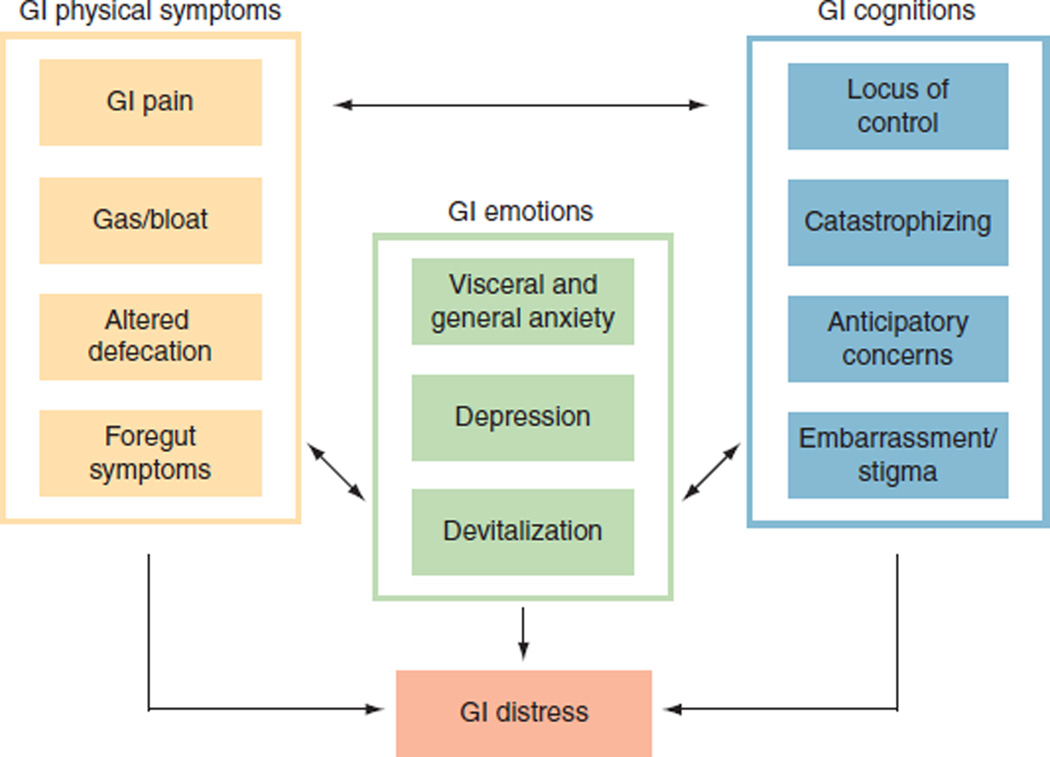
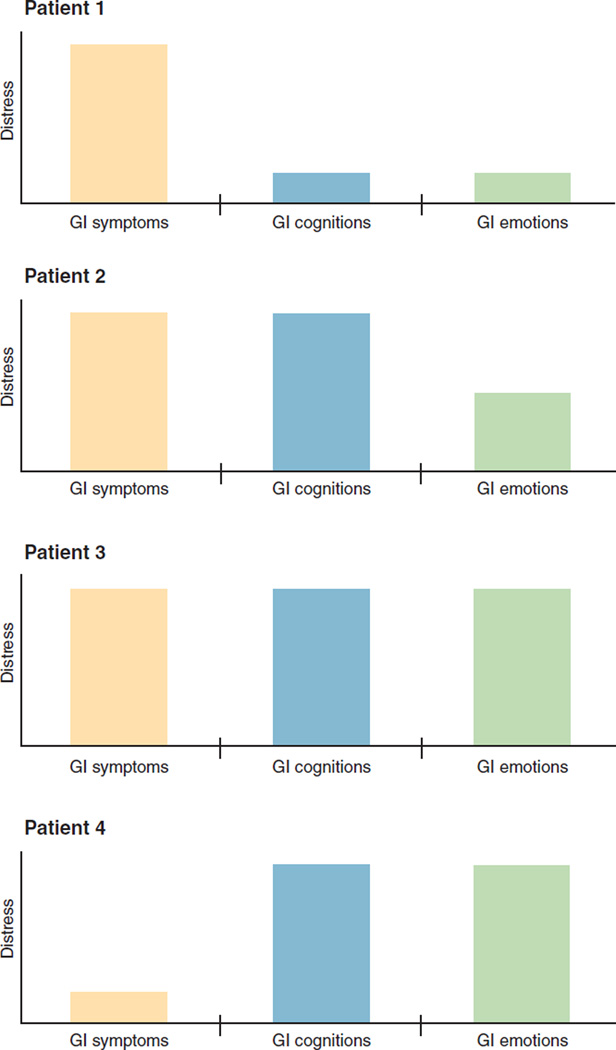
We describe a framework to help clinicians think about health-related quality of life in their gastrointestinal (GI) patients. We introduce "GI distress" as a clinically relevant concept and explain how it may result from physical symptoms, cognitions, and emotions. The GI distress framework suggests that providers should divide GI physical symptoms into four categories: pain, gas/bloat, altered defecation, and foregut symptoms. We describe how these physical symptoms can be amplified by maladaptive cognitions, including external locus of control, catastrophizing, and anticipation anxiety. We suggest determining the level of embarrassment from GI symptoms and asking about stigmatization. GI patients may also harbor emotional distress from their illness and may exhibit visceral anxiety marked by hypervigilance, fear, and avoidance of GI sensations. Look for signs of devitalization, indicated by inappropriate fatigue. When appropriate, screen for suicidal ideations. Finally, we provide a list of high-yield questions to screen for these maladaptive cognitions and emotions, and explain how the GI distress framework can be used in clinical practice.
Figures
References
-
- Eisen GM, Locke GR, 3rd, Provenzale D. Health-related quality of life: a primer for gastroenterologists. Am J Gastroenterol. 1999;94:2017–2021. - PubMed
-
- Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med. 1993;118:622–629. - PubMed
-
- Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113:9–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
