

Management of diabetes and associated cardiovascular risk factors in seven countries: a comparison of data from national health examination surveys
- PMID: 21379413
- PMCID: PMC3044248
- DOI: 10.2471/BLT.10.080820
Management of diabetes and associated cardiovascular risk factors in seven countries: a comparison of data from national health examination surveys
Abstract
Objective: To examine the effectiveness of the health system response to the challenge of diabetes across different settings and explore the inequalities in diabetes care that are attributable to socioeconomic factors.
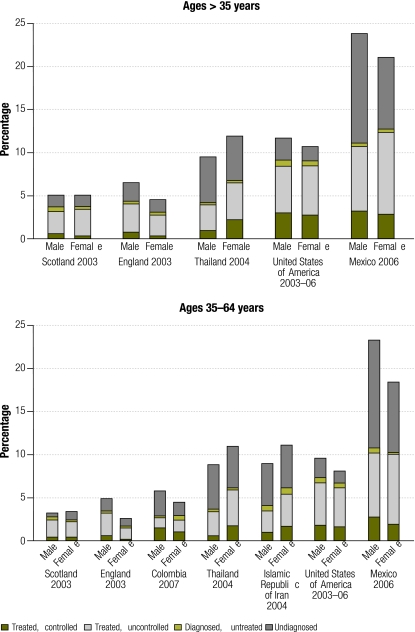
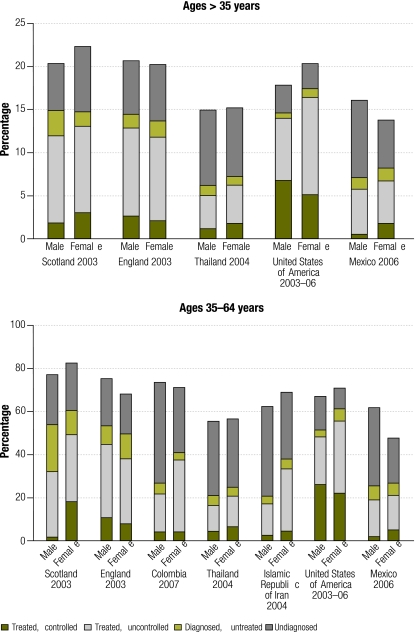
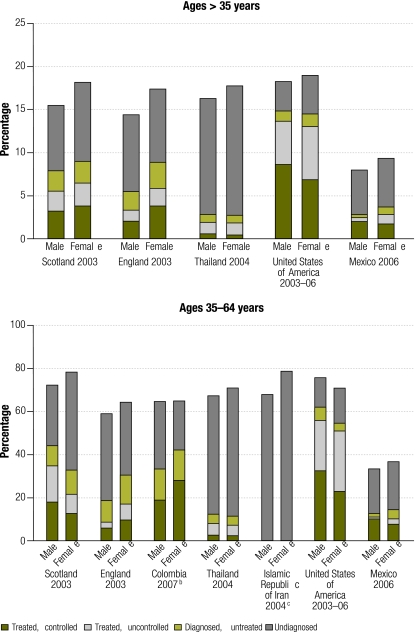
Methods: We used nationally representative health examination surveys from Colombia, England, the Islamic Republic of Iran, Mexico, Scotland, Thailand and the United States of America to obtain data on diagnosis, treatment and control of hyperglycaemia, arterial hypertension and hypercholesterolaemia among individuals with diabetes. Using logistic regression, we explored the socioeconomic determinants of diagnosis and effective case management.
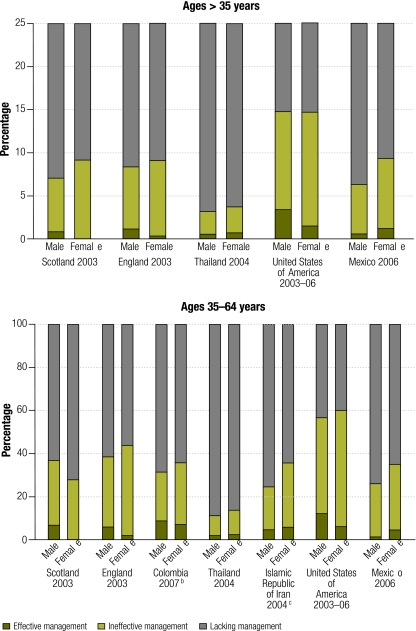
Findings: A substantial proportion of individuals with diabetes remain undiagnosed and untreated, both in developed and developing countries. The figures range from 24% of the women in Scotland and the USA to 62% of the men in Thailand. The proportion of individuals with diabetes reaching treatment targets for blood glucose, arterial blood pressure and serum cholesterol was very low, ranging from 1% of male patients in Mexico to about 12% in the United States. Income and education were not found to be significantly related to the rates of diagnosis and treatment anywhere except in Thailand, but in the three countries with available data insurance status was a strong predictor of diagnosis and effective management, especially in the United States.
Conclusion: There are many missed opportunities to reduce the burden of diabetes through improved control of blood glucose levels and improved diagnosis and treatment of arterial hypertension and hypercholesterolaemia. While no large socioeconomic inequalities were noted in the management of individuals with diabetes, financial access to care was a strong predictor of diagnosis and management.
Objectif: Étudier l'efficacité de la réponse du système de santé au problème du diabète sur différents paramètres et explorer les inégalités dans la prise en charge du diabète, attribuables à des facteurs socio-économiques.
Méthodes: Nous avons utilisé des enquêtes de santé par examen représentatives au plan national pour la Colombie, l'Angleterre, la République islamique d'Iran, le Mexique, l'Écosse, la Thaïlande et les États-Unis d'Amérique. Les données exploitées portent sur le diagnostic, le traitement et le contrôle de l'hyperglycémie, de l'hypertension artérielle et de l’hypercholestérolémie chez les diabétiques. Nous avons utilisé la régression logistique pour explorer les déterminants socioéconomiques du diagnostic et de la bonne gestion thérapeutique.
Résultats: Une proportion substantielle des diabétiques n’a pas fait l’objet d’un diagnostic et ne reçoit par conséquent aucun traitement et ce, à la fois dans les pays développés et dans les pays en voie de développement. Les chiffres vont de 24% des femmes en Écosse et aux États-Unis d’Amérique à 62% des hommes en Thaïlande. La proportion de diabétiques atteignant les cibles de traitement pour la glycémie, la tension artérielle et le cholestérol sérique était très faible: de 1% des patients masculins au Mexique jusqu'à environ 12% aux États-Unis. Il n’a pas été constaté que le revenu et l'éducation aient un lien significatif avec les taux de diagnostic et de traitement sauf en Thaïlande. Toutefois, pour les trois pays pour lesquels nous disposions de données, la couverture sociale était un puissant indicateur de diagnostic et de traitement efficace, particulièrement aux États-Unis.
Conclusion: Il existe de nombreuses occasions manquées de réduction du fardeau du diabète au moyen d'un contrôle renforcé des taux de glycémie et d'un diagnostic et d'un traitement meilleurs de l'hypertension artérielle et de l'hypercholestérolémie. Alors qu'aucune inégalité socioéconomique importante n'a été relevée dans le traitement des diabétiques, le coût de l'accès aux soins s'est révélé être un puissant indicateur de diagnostic et de traitement.
Objetivo: Examinar la efectividad de la respuesta del sistema sanitario ante el reto de la diabetes en diversos entornos y observar las desigualdades atribuibles a factores socioeconómicos en el tratamiento de la diabetes.
Métodos: Hemos empleado las encuestas representativas a nivel nacional de los exámenes médicos de Colombia, Escocia, Estados Unidos, Inglaterra, México, la República Islámica de Irán y Tailandia para obtener datos sobre el diagnóstico, el tratamiento y el control de la hiperglucemia, la hipertensión arterial y la hipercolesterolemia en pacientes con diabetes. Empleando una regresión logística, hemos analizado los determinantes socioeconómicos del diagnóstico y de un tratamiento efectivo de cada caso.
Resultados: Un proporción considerable de pacientes con diabetes permanecen sin diagnosticar y sin tratar, tanto en los países desarrollados como en aquellos en vías de desarrollo. Las cifras oscilan desde un 24% de las mujeres en Escocia y Estados Unidos hasta un 62% de los hombres en Tailandia. Solo una proporción muy reducida de personas con diabetes (oscilando entre el 1% de los pacientes hombres en México y alrededor del 12% en Estados Unidos) alcanzó los objetivos de su tratamiento para sus problemas de glucosa en sangre, presión arterial y nivel sérico de colesterol. En ninguna de las regiones (excepto Tailandia) se observó que los porcentajes de diagnóstico y tratamiento estuvieran relacionados con los ingresos y la educación, si bien en tres países con datos disponibles contar con un seguro representó un factor importante de previsibilidad para el diagnóstico y tratamiento efectivo de la diabetes, especialmente en el caso de Estados Unidos.
Conclusión: Se han dejado pasar muchas oportunidades para reducir la carga de la diabetes a través de un mejor control de los niveles de glucosa en sangre y de un mejor diagnóstico y tratamiento de la hipertensión arterial y de la hipercolesterolemia. Si bien no se observaron grandes desigualdades socioeconómicas en el tratamiento de los pacientes con diabetes, el acceso económico al tratamiento fue un factor importante de previsibilidad para el diagnóstico y el tratamiento de esta enfermedad.
الغرض: فحص فعالية تصدي النظام الصحي لتحدي السكري في مواقع مختلفة واستكشاف عدم المساواة في رعاية السكري التي تُعزَى إلى عوامل اجتماعية واقتصادية.
الطريقة: استخدم الباحثون مسوحات وطنية لفحص الصحة من كل من كمبوديا، وانكلترا، وجمهورية إيران الإسلامية، والمكسيك، وسكوتلاندا، وتايلاند، والولايات المتحدة الأمريكية لجمع معطيات تشخيص، ومعالجة، وتضبيط فرط سكر الدم، وفرط الضغط الشرياني، وفرط كوليستيرول الدم بين المصابين بالسكري. واستكشف الباحثون، باستخدام التحوّف اللوجستي، المحددات الاجتماعية-الاقتصادية للتشخيص والتدبير العلاجي الفعّال للحالات.
النتائج: لم تُشخَّص ولم تعالج نسبة كبيرة من المصابين بالسكري، في كل من البلدان المتقدمة والنامية. وتراوحت هذه النسبة من24% بين النساء في سكوتلاندا والولايات المتحدة الأمريكية إلى% 62 بين الرجال في تايلاند. وكانت نسبة المصابين بالسكري الذين بلغوا مرامي معالجة غلوكوز الدم، وضغط الدم الشرياني، والكوليستيرول المصلي نسبة منخفضة للغاية، تراوحت بين% 1 من الذكور في المكسيك إلى % 12 في الولايات المتحدة. لم يُلاحَظ للدخل والتعليم علاقة يعتد بها إحصائياً مع معدلات التشخيص والمعالجة في أي مكان ماعدا تايلاند، وكانت حالة التأمين، في ثلاثة بلدان توفرت فيها المعطيات، منبئاً قوياً على التشخيص وفعالية التدبير العلاجي، ولاسيما في الولايات المتحدة.
الاستنتاج: كثير من الفرص المفقودة يمكن الاستفادة منها للحد من عبء السكري عن طريق تحسين تضبيط مستويات غلوكوز الدم، وتحسين تشخيص ومعالجة فرط الضغط الشرياني وفرط كوليستيرول الدم. ومع أنه لم يُلاحَظ في التدبير العلاجي للمصابين بالسكري قدر كبير من عدم المساواة الاقتصادية والاجتماعية، إلا أن القدرة المالية على الوصول إلى خدمات الرعاية كانت منبئاً قوياً على التشخيص والتدبير العلاجي.
Цель: Рассмотреть эффективность реакции системы здравоохранения на проблему диабета в различных условиях и исследовать неравенство в области медико-санитарной помощи при диабете, обусловленное социально-экономическими факторами.
Методы: Для получения данных о диагностике, лечении и контроле гипергликемии, артериальной гипертензии и повышенного уровня холестерина среди больных диабетом мы использовали данные национально-репрезентативных опросов по изучению состояния здоровья, проводившихся в Англии, Исламской Республике Иран, Колумбии, Мексике, Соединенных Штатах Америки, Таиланде и Шотландии. Используя логистическую регрессию, мы исследовали социально-экономические детерминанты диагностики и эффективного лечения больных.
Результаты: Как в развитых, так и в развивающихся странах у значительной доли больных диабет не диагностируется, и они не получают лечения. Цифры варьируют от 24% женщин в Шотландии до 62% мужчин в Таиланде. Доля больных диабетом, достигающих целей лечения в отношении содержания глюкозы в крови, артериального кровяного давления и сывороточного холестерина, была очень низкой и ранжировала от 1% пациентов-мужчин в Мексике до примерно 12% в США. Нигде, за исключением Таиланда, не было выявлено существенной корреляции между доходом, образованием и показателями диагностирования и лечения. Однако в трех странах, данные по которым были доступны, особенно в США, сильным предиктором диагностирования и эффективного ведения диабета являлся страховой статус.
Вывод: Существует много неиспользованных возможностей для снижения бремени заболеваемости диабетом путем улучшения контроля над уровнем содержания глюкозы в крови, а также совершенствования диагностики и лечения артериальной гипертензии и повышенного уровня холестерина. Хотя значительного социально-экономического неравенства в ведении больных диабетом отмечено не было, финансовая доступность медико-санитарной помощи являлась сильным предиктором диагностики и эффективного лечения болезни.
目的: 旨在考察不同环境下的医疗体系应对糖尿病挑战的有效性,并探讨因社会经济因素引起的糖尿病护理中的不平等现象。
方法: 我们运用哥伦比亚、英格兰、伊朗、墨西哥、苏格兰、泰国和美国的全国代表性体检调查结果,从中获得糖尿病患者在诊断、治疗和高血糖、动脉高血压和高胆固醇血症的控制方面的数据。使用逻辑回归分析探讨了诊断和病例有效管理的社会经济因素。
结果: 无论是在发达国家还是在发展中国家,有相当比例的糖尿病患者仍然未经诊断和治疗。这方面数字在24%(苏格兰和美国女性)到62%(泰国男性)之间变化。实现血糖、动脉血压和胆固醇治疗目标的糖尿病患者的比例非常低,仅占1%(墨西哥男性)到约12%(美国)。除泰国外,未发现收入和教育程度与诊断和治疗比例显著相关。然而,在有可用数据的三个国家,特别是在美国,保险状况是实现糖尿病诊断和有效管理的一个强大的预警器。
结论: 人们错过了很多通过更好地控制血糖水平、更早地诊断和治疗动脉高血压和高胆固醇血症来减轻糖尿病负担的机会。尽管在糖尿病患者的管理中并未发现重大经济社会不公现象,但是,具备享受医疗服务的经济能力仍是实现糖尿病诊断和有效管理的一个强大预警器。
Figures
References
-
- Aekplakorn W, Abbott-Klafter J, Premgamone A, Dhanamun B, Chaikittiporn C, Chongsuvivatwong V, et al. Prevalence and management of diabetes and associated risk factors by regions of Thailand: Third National Health Examination Survey 2004. Diabetes Care. 2007;30:2007–12. doi: 10.2337/dc06-2319. - DOI - PubMed
-
- Gu D, Reynolds K, Duan X, Xin X, Chen J, Wu X, et al. InterASIA Collaborative Group Prevalence of diabetes and impaired fasting glucose in the Chinese adult population: International Collaborative Study of Cardiovascular Disease in Asia (InterASIA). Diabetologia. 2003;46:1190–8. doi: 10.1007/s00125-003-1167-8. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical