

Seropositivity to cytomegalovirus, inflammation, all-cause and cardiovascular disease-related mortality in the United States
- PMID: 21379581
- PMCID: PMC3040745
- DOI: 10.1371/journal.pone.0016103
Seropositivity to cytomegalovirus, inflammation, all-cause and cardiovascular disease-related mortality in the United States
Abstract
Background: Studies have suggested that CMV infection may influence cardiovascular disease (CVD) risk and mortality. However, there have been no large-scale examinations of these relationships among demographically diverse populations. The inflammatory marker C-reactive protein (CRP) is also linked with CVD outcomes and mortality and may play an important role in the pathway between CMV and mortality. We utilized a U.S. nationally representative study to examine whether CMV infection is associated with all-cause and CVD-related mortality. We also assessed whether CRP level mediated or modified these relationships.
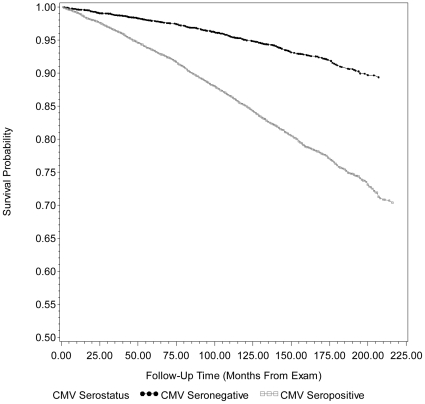
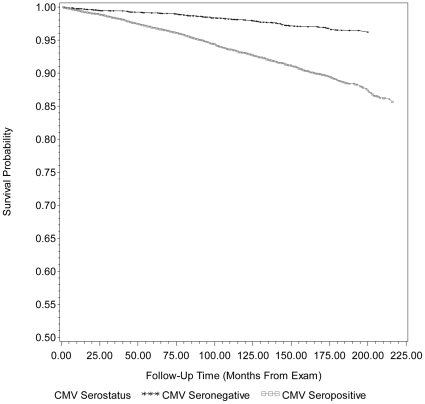
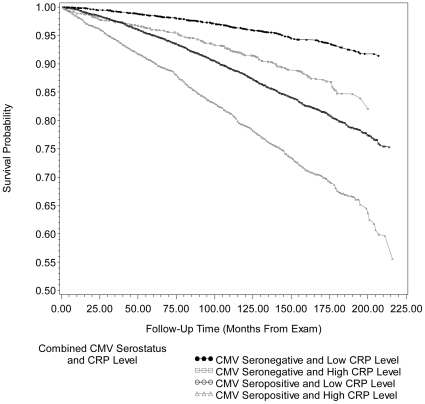
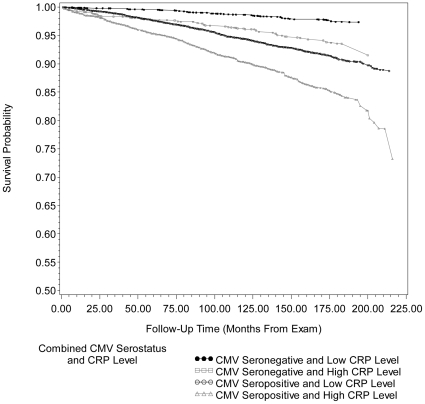
Methodology/principal findings: Data come from subjects ≥ 25 years of age who were tested for CMV and CRP level and were eligible for mortality follow-up on December 31(st), 2006 (N = 14153) in the National Health and Nutrition Examination Survey (NHANES) III (1988-1994). Cox proportional hazard models were used to estimate hazard ratios (HR) and 95% confidence intervals (CI) for all-cause and CVD-related mortality by CMV serostatus. After adjusting for multiple confounders, CMV seropositivity remained statistically significantly associated with all-cause mortality (HR 1.19, 95% CI: 1.01, 1.41). The association between CMV and CVD-related mortality did not achieve statistical significance after confounder adjustment. CRP did not mediate these associations. However, CMV seropositive individuals with high CRP levels showed a 30.1% higher risk for all-cause mortality and 29.5% higher risk for CVD-related mortality compared to CMV seropositive individuals with low CRP levels.
Conclusions/significance: CMV was associated with a significant increased risk for all-cause mortality and CMV seropositive subjects who also had high CRP levels were at substantially higher risk for both for all-cause and CVD-related mortality than subjects with low CRP levels. Future work should target the mechanisms by which CMV infection and low-level inflammation interact to yield significant impact on mortality.
Conflict of interest statement
Figures
References
-
- Staras SA, Dollard SC, Radford KW, Flanders WD, Pass RF, et al. Seroprevalence of cytomegalovirus infection in the United States, 1988–1994. Clin Infect Dis. 2006;43:1143–1151. - PubMed
-
- Britt W. Human Cytomegalovirus; 2008. Manifestations of human cytomegalovirus infection: proposed mechanisms of acute and chronic disease. pp. 417–470. - PubMed
-
- Mocarski ES, Jr, Hahn G, Lofgren White K, Xu J, Slobedman B, et al. Myeloid Cell Recruitment and Function in Pathogenesis and Latency. In: Reddehase MJ, editor. Cytomegaloviruses: Molecular Biology and Immunology. Norfolk, UK: Caister Academic Press; 2006. pp. 465–482.
-
- Nieto FJ, Adam E, Sorlie P, Farzadegan H, Melnick JL, et al. Cohort study of cytomegalovirus infection as a risk factor for carotid intimal-medial thickening, a measure of subclinical atherosclerosis. Circulation. 1996;94:922–927. - PubMed
-
- Sorlie PD, Nieto FJ, Adam E, Folsom AR, Shahar E, et al. A Prospective Study of Cytomegalovirus, Herpes Simplex Virus 1, and Coronary Heart Disease: The Atherosclerosis Risk in Communities (ARIC) Study. Arch Intern Med. 2000;160:2027–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
