

The effects of levosimendan and glibenclamide on circulatory and metabolic variables in a canine model of acute hypoxia
- PMID: 21380525
- PMCID: PMC3058361
- DOI: 10.1007/s00134-011-2144-1
The effects of levosimendan and glibenclamide on circulatory and metabolic variables in a canine model of acute hypoxia
Abstract
Purpose: To study the effects of pretreatment with levosimendan (LEVO, a Ca²(+)-sensitizer and K (ATP) (+) channel opener) and/or the K (ATP) (+) channel antagonist glibenclamide (GLIB) on systemic hemodynamics, metabolism, and regional gastromucosal oxygenation during hypoxic hypoxemia.
Methods: Chronically instrumented, healthy dogs (24-32 kg, n = 6 per group, randomized cross-over design) were repeatedly sedated, mechanically ventilated (FiO₂ ~0.3) and subjected to the following interventions: no pretreatment, LEVO pretreatment, GLIB pretreatment, or combined LEVO + GLIB pretreatment, each followed by hypoxic hypoxemia (FiO₂ ~0.1). We measured cardiac output (CO, ultrasonic flow probes), oxygen consumption (VO₂, indirect calorimetry), and gastromucosal microvascular hemoglobin oxygenation (μHbO₂, spectrophotometry).
Statistics: data are presented as mean ± SEM and compared by one-way ANOVA (direct drug effects within group) and two-way ANOVA (between all hypoxic conditions) both with Bonferroni corrections; p < 0.05.
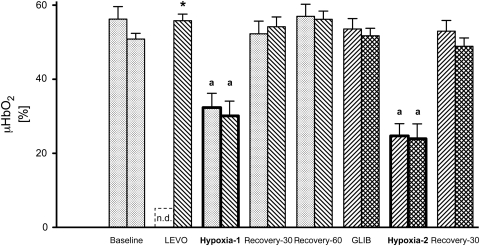
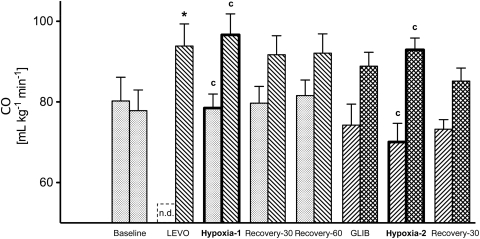
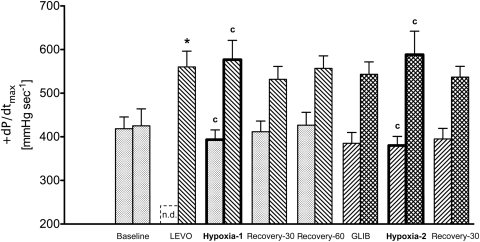
Results: In LEVO-pretreated hypoxemia, CO was significantly higher compared to unpretreated hypoxemia. The increased CO was neither associated with an increased VO₂ nor with markers of aggravated anaerobiosis (pH, BE, lactate). In addition, LEVO pretreatment did not further compromise gastromucosal μHbO₂ in hypoxemia. After combined LEVO + GLIB pretreatment, systemic effects of GLIB were apparent, however, CO was significantly higher than during unpretreated and GLIB-pretreated hypoxemia, but equal to LEVO-pretreated hypoxemia, indicating that GLIB did not prevent the increased CO in LEVO-pretreated hypoxia.
Conclusions: LEVO pretreatment resulted in improved systemic circulation (CO) during hypoxemia without fueling systemic VO₂, without aggravating systemic anaerobiosis markers, and without further compromising microvascular gastromucosal oxygenation. Thus, LEVO pretreatment may be an option to support the systemic circulation during hypoxia.
Figures
Comment in
-
Levosimendan: from coronary care to intensive care?Intensive Care Med. 2011 Apr;37(4):569-71. doi: 10.1007/s00134-011-2204-6. Epub 2011 Mar 5. Intensive Care Med. 2011. PMID: 21380519 No abstract available.
References
-
- Hilbert G, Gruson D, Vargas F, Valentino R, Favier JC, Portel L, Gbikpi-Benissan G, Cardinaud JP. Bronchoscopy with bronchoalveolar lavage via the laryngeal mask airway in high-risk hypoxemic immunosuppressed patients. Crit Care Med. 2001;29:249–255. doi: 10.1097/00003246-200102000-00004. - DOI - PubMed
-
- Jaber S, Amraoui J, Lefrant JY, Arich C, Cohendy R, Landreau L, Calvet Y, Capdevila X, Mahamat A, Eledjam JJ. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit. Crit Care Med. 2006;34:2355–2361. doi: 10.1097/01.CCM.0000233879.58720.87. - DOI - PubMed
-
- Sud S, Friedrich JO, Taccone P, Polli F, Adhikari NK, Latini R, Pesenti A, Guérin C, Mancebo J, Curley MA, Fernandez R, Chan MC, Beuret P, Voggenreiter G, Sud M, Tognoni G, Gattinoni L. Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia. Intensive Care Med. 2010;36:585–599. doi: 10.1007/s00134-009-1748-1. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
