

Second-phase hepatitis C virus RNA decline during telaprevir-based therapy increases with drug effectiveness: implications for treatment duration
- PMID: 21384401
- PMCID: PMC3103645
- DOI: 10.1002/hep.24272
Second-phase hepatitis C virus RNA decline during telaprevir-based therapy increases with drug effectiveness: implications for treatment duration
Abstract
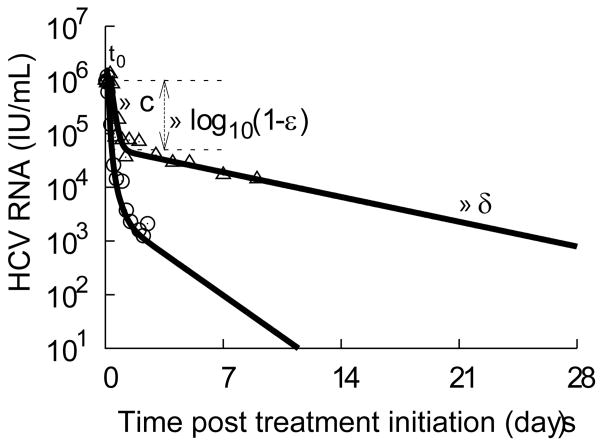
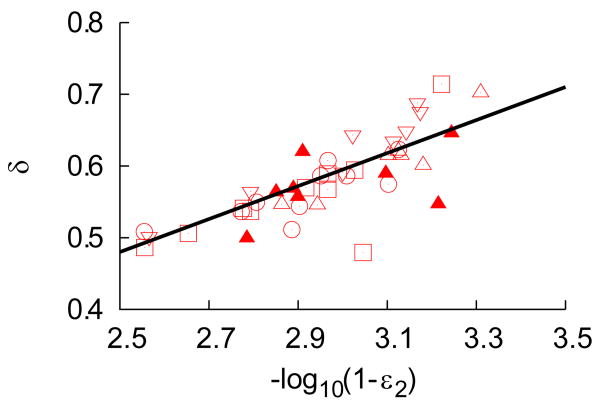
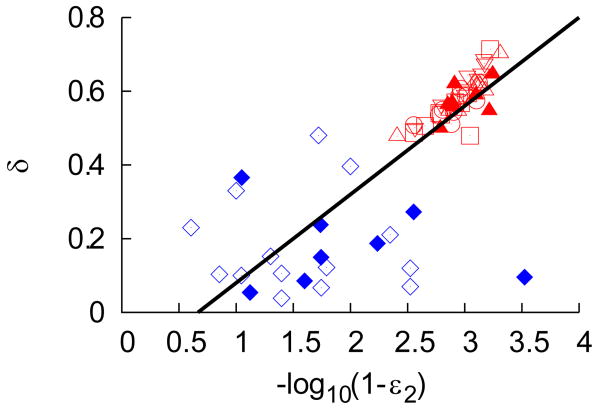
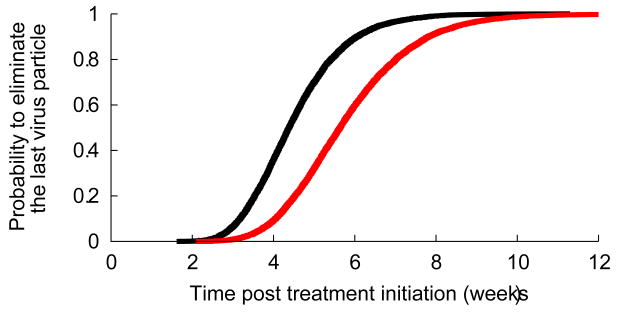
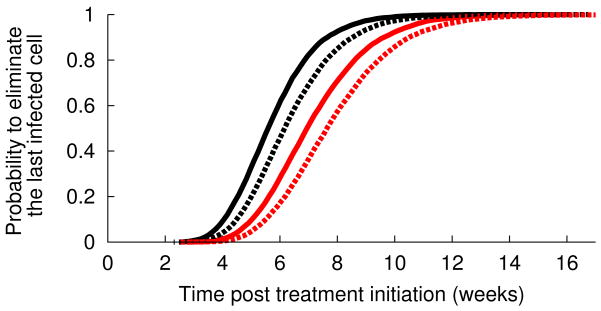
Hepatitis C virus (HCV) RNA decay during antiviral therapy is characterized by a rapid first phase, followed by a slower second phase. The current understanding of viral kinetics attributes the magnitude of the first phase of decay to treatment effectiveness, whereas the second phase of decay is attributed to the progressive loss of infected cells. Here, we analyzed data from 44 patients treated with telaprevir, a potent HCV protease inhibitor. Using a viral kinetic model that accounts for the pharmacokinetics of telaprevir, we found the second-phase slope of viral decline to be strongly correlated with treatment effectiveness and to be roughly four-fold more rapid than has been reported with interferon-based therapies. Because telaprevir is not known to increase the death rate of infected cells, our results suggest that the second-phase slope of viral decline is driven not only by the death of infected cells, but may also involve other mechanisms, such as a treatment-effectiveness-dependent degradation of intracellular viral RNA. As a result of the enhanced viral decay caused by the high antiviral effectiveness of telaprevir, we predict that if drug resistance could be avoided by using an appropriate combination of antiviral agents, treatment duration needed to clear HCV might be dramatically shortened. Indeed, we predict that in 95% of fully compliant patients, the last virus particle should be eliminated by week 7 of therapy. If the remaining infected hepatocytes act as a potential reservoir for the renewal of infection, no more than 10 weeks of treatment should be sufficient to clear the infection in 95% of fully compliant patients. However, if patients miss doses, treatment duration would need to be extended.
Copyright © 2011 American Association for the Study of Liver Diseases.
Figures
References
-
- Hepatitis C fact sheet. [Accessed July 13, 2009]; Available from: http://www.who.int/mediacentre/factsheets/fs164/en/
-
- Neumann AU, Lam NP, Dahari H, Gretch DR, Wiley TE, Layden TJ, Perelson AS. Hepatitis C viral dynamics in vivo and the antiviral efficacy of interferon-alpha therapy. Science. 1998;282:103–107. - PubMed
-
- Dixit NM, Layden-Almer JE, Layden TJ, Perelson AS. Modelling how ribavirin improves interferon response rates in hepatitis C virus infection. Nature. 2004;432:922–924. - PubMed
-
- Pilli M, Zerbini A, Penna A, Orlandini A, Lukasiewicz E, Pawlotsky J, Zeuzem S, et al. HCV-specific T-cell response in relation to viral kinetics and treatment outcome (DITTO-HCV project) Gastroenterology. 2007;133:1132–1143. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials