

Vascular pedicle width in acute lung injury: correlation with intravascular pressures and ability to discriminate fluid status
- PMID: 21385351
- PMCID: PMC3219344
- DOI: 10.1186/cc10084
Vascular pedicle width in acute lung injury: correlation with intravascular pressures and ability to discriminate fluid status
Abstract
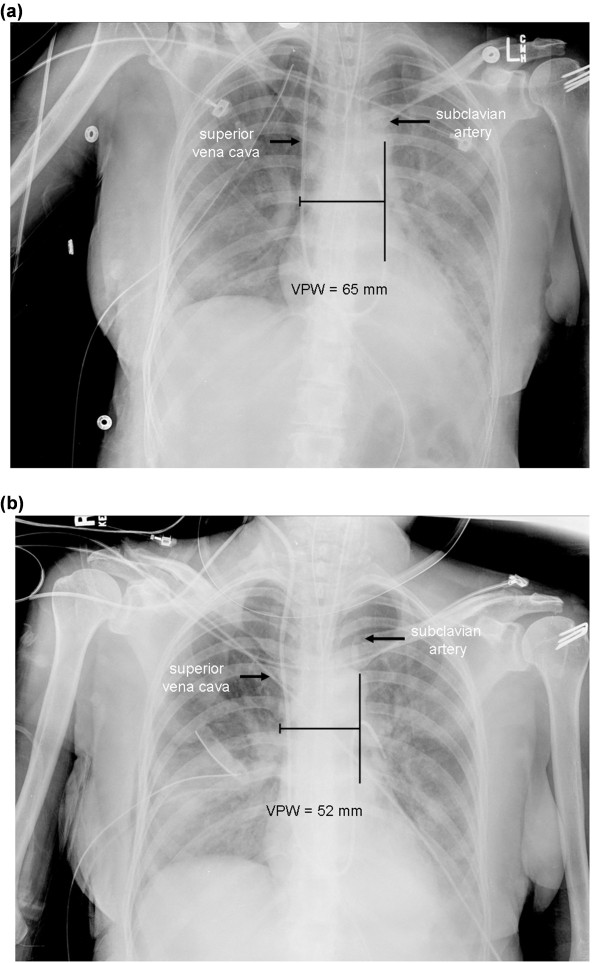
Introduction: Conservative fluid management in patients with acute lung injury (ALI) increases time alive and free from mechanical ventilation. Vascular pedicle width (VPW) is a non-invasive measurement of intravascular volume status. The VPW was studied in ALI patients to determine the correlation between VPW and intravascular pressure measurements and whether VPW could predict fluid status.
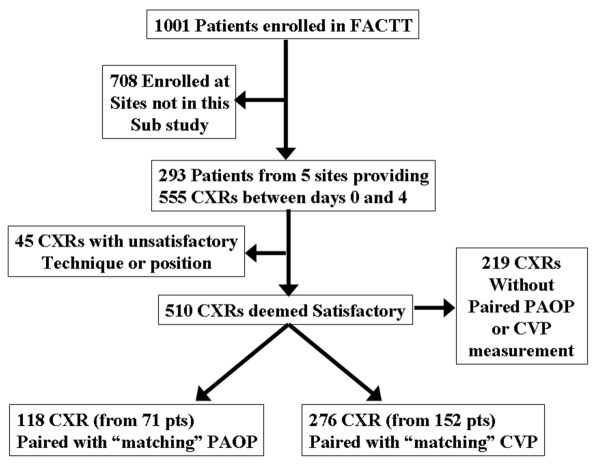
Methods: This retrospective cohort study involved 152 patients with ALI enrolled in the Fluid and Catheter Treatment Trial (FACTT) from five NHLBI ARDS (Acute Respiratory Distress Syndrome) Network sites. VPW and central venous pressure (CVP) or pulmonary artery occlusion pressure (PAOP) from the first four study days were correlated. The relationships between VPW, positive end-expiratory pressure (PEEP), cumulative fluid balance, and PAOP were also evaluated. Receiver operator characteristic (ROC) curves were used to determine the ability of VPW to detect PAOP < 8 mmHg and PAOP ≥ 18 mm Hg.
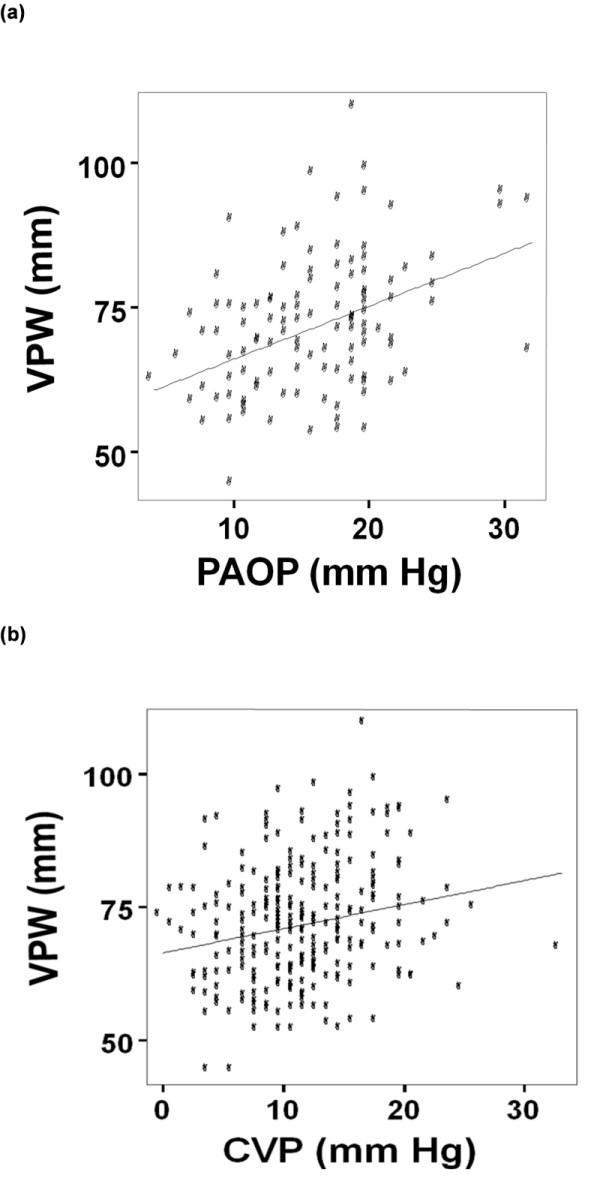
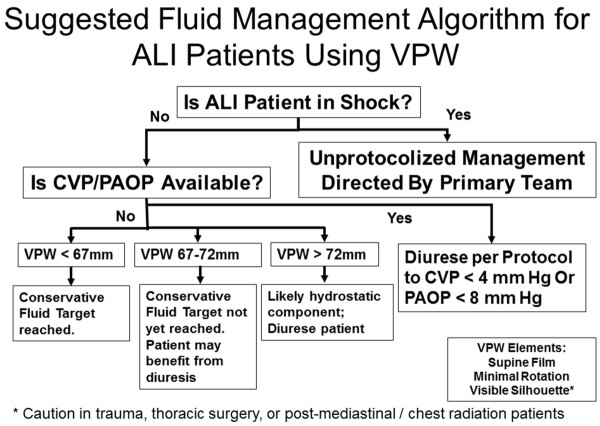
Results: A total of 71 and 152 patients provided 118 and 276 paired VPW/PAOP and VPW/CVP measurements, respectively. VPW correlated with PAOP (r = 0.41; P < 0.001) and less well with CVP (r = 0.21; P = 0.001). In linear regression, VPW correlated with PAOP 1.5-fold better than cumulative fluid balance and 2.5-fold better than PEEP. VPW discriminated achievement of PAOP < 8 mm Hg (AUC = 0.73; P = 0.04) with VPW ≤67 mm demonstrating 71% sensitivity (95% CI 30 to 95%) and 68% specificity (95% CI 59 to 75%). For discriminating a hydrostatic component of the edema (that is, PAOP ≥ 18 mm Hg), VPW ≥ 72 mm demonstrated 61.4% sensitivity (95% CI 47 to 74%) and 61% specificity (49 to 71%) (area under the curve (AUC) 0.69; P = 0.001).
Conclusions: VPW correlates with PAOP better than CVP in patients with ALI. Due to its only moderate sensitivity and specificity, the ability of VPW to discriminate fluid status in patients with acute lung injury is limited and should only be considered when intravascular pressures are unavailable.
Figures

References
-
- Antonelli M, Levy M, Andrews PJ, Chastre J, Hudson LD, Manthous C, Meduri GU, Moreno RP, Putensen C, Stewart T, Torres A. Hemodynamic monitoring in shock and implications for management. International Consensus Conference, Paris, France, 27-28 April 2006. Intensive Care Med. 2007;33:575–590. doi: 10.1007/s00134-007-0531-4. - DOI - PubMed
-
- Milne EN, Pistolesi M, Miniati M, Giuntini C. The vascular pedicle of the heart and the vena azygos. Part I: The normal subject. Radiology. 1984;152:1–8. - PubMed
