

Arterial hyperoxia and in-hospital mortality after resuscitation from cardiac arrest
- PMID: 21385416
- PMCID: PMC3219350
- DOI: 10.1186/cc10090
Arterial hyperoxia and in-hospital mortality after resuscitation from cardiac arrest
Abstract
Introduction: Hyperoxia has recently been reported as an independent risk factor for mortality in patients resuscitated from cardiac arrest. We examined the independent relationship between hyperoxia and outcomes in such patients.
Methods: We divided patients resuscitated from nontraumatic cardiac arrest from 125 intensive care units (ICUs) into three groups according to worst PaO2 level or alveolar-arterial O2 gradient in the first 24 hours after admission. We defined 'hyperoxia' as PaO2 of 300 mmHg or greater, 'hypoxia/poor O2 transfer' as either PaO2 < 60 mmHg or ratio of PaO2 to fraction of inspired oxygen (FiO2 ) < 300, 'normoxia' as any value between hypoxia and hyperoxia and 'isolated hypoxemia' as PaO2 < 60 mmHg regardless of FiO2. Mortality at hospital discharge was the main outcome measure.
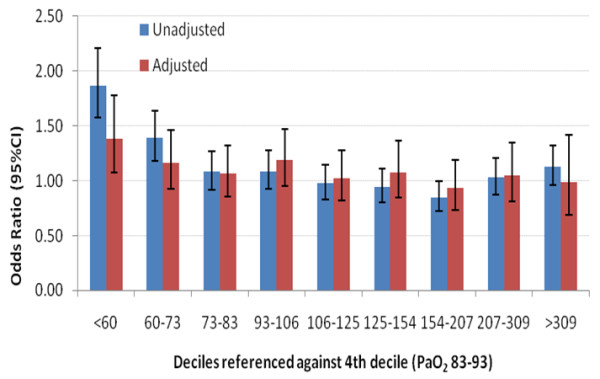
Results: Of 12,108 total patients, 1,285 (10.6%) had hyperoxia, 8,904 (73.5%) had hypoxia/poor O2 transfer, 1,919 (15.9%) had normoxia and 1,168 (9.7%) had isolated hypoxemia (PaO2 < 60 mmHg). The hyperoxia group had higher mortality (754 (59%) of 1,285 patients; 95% confidence interval (95% CI), 56% to 61%) than the normoxia group (911 (47%) of 1,919 patients; 95% CI, 45% to 50%) with a proportional difference of 11% (95% CI, 8% to 15%), but not higher than the hypoxia group (5,303 (60%) of 8,904 patients; 95% CI, 59% to 61%). In a multivariable model controlling for some potential confounders, including illness severity, hyperoxia had an odds ratio for hospital death of 1.2 (95% CI, 1.1 to 1.6). However, once we applied Cox proportional hazards modelling of survival, sensitivity analyses using deciles of hypoxemia, time period matching and hyperoxia defined as PaO2 > 400 mmHg, hyperoxia had no independent association with mortality. Importantly, after adjustment for FiO2 and the relevant covariates, PaO2 was no longer predictive of hospital mortality (P = 0.21).
Conclusions: Among patients admitted to the ICU after cardiac arrest, hyperoxia did not have a robust or consistently reproducible association with mortality. We urge caution in implementing policies of deliberate decreases in FiO2 in these patients.
Figures
Comment in
-
How to assess the dangers of hyperoxemia: methodological issues.Crit Care. 2011;15(3):435; author reply 435. doi: 10.1186/cc10272. Epub 2011 Jun 30. Crit Care. 2011. PMID: 21722333 Free PMC article. No abstract available.
-
Hyperoxia after cardiac arrest may not increase ischemia-reperfusion injury.Crit Care. 2011;15(3):166. doi: 10.1186/cc10250. Epub 2011 Jun 22. Crit Care. 2011. PMID: 21722351 Free PMC article.
References
-
- Peberdy MA, Kaye W, Ornato JP, Larkin GL, Nadkarni V, Mancini ME, Berg RA, Nichol G, Lane-Trultt T. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297–308. doi: 10.1016/S0300-9572(03)00215-6. - DOI - PubMed
-
- Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, Nichol G, Cousineau D, Blackburn J, Munkley D, Luinstra-Toohey L, Campeau T, Dagnone E, Lyver M. Ontario Prehospital Advanced Life Support Study Group. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351:647–656. doi: 10.1056/NEJMoa040325. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
