

Acute respiratory failure in kidney transplant recipients: a multicenter study
- PMID: 21385434
- PMCID: PMC3219351
- DOI: 10.1186/cc10091
Acute respiratory failure in kidney transplant recipients: a multicenter study
Abstract
Introduction: Data on pulmonary complications in renal transplant recipients are scarce. The aim of this study was to evaluate acute respiratory failure (ARF) in renal transplant recipients.
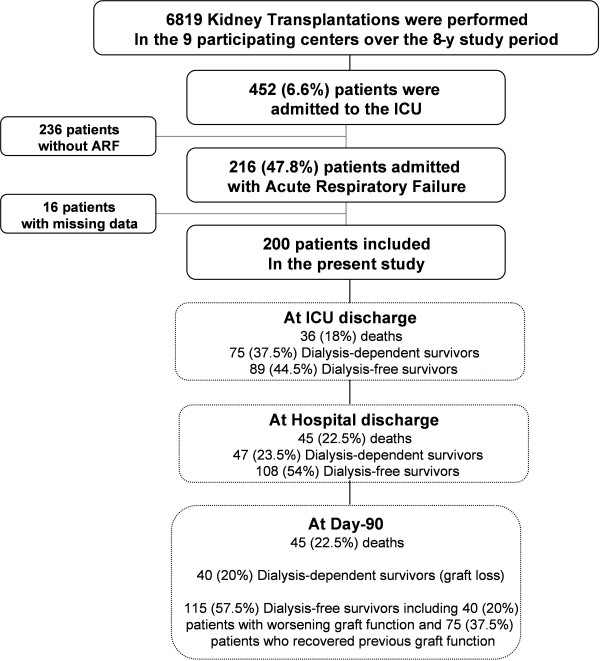
Methods: We conducted a retrospective observational study in nine transplant centers of consecutive kidney transplant recipients admitted to the intensive care unit (ICU) for ARF from 2000 to 2008.
Results: Of 6,819 kidney transplant recipients, 452 (6.6%) required ICU admission, including 200 admitted for ARF. Fifteen (7.5%) of these patients had combined kidney-pancreas transplantations. The most common causes of ARF were bacterial pneumonia (35.5%), cardiogenic pulmonary edema (24.5%) and extrapulmonary acute respiratory distress syndrome (ARDS) (15.5%). Pneumocystis pneumonia occurred in 11.5% of patients. Mechanical ventilation was used in 93 patients (46.5%), vasopressors were used in 82 patients (41%) and dialysis was administered in 104 patients (52%). Both the in-hospital and 90-day mortality rates were 22.5%. Among the 155 day 90 survivors, 115 patients (74.2%) were dialysis-free, including 75 patients (65.2%) who recovered prior renal function. Factors independently associated with in-hospital mortality were shock at admission (odds ratio (OR) 8.70, 95% confidence interval (95% CI) 3.25 to 23.29), opportunistic fungal infection (OR 7.08, 95% CI 2.32 to 21.60) and bacterial infection (OR 2.53, 95% CI 1.07 to 5.96). Five factors were independently associated with day 90 dialysis-free survival: renal Sequential Organ Failure Assessment (SOFA) score on day 1 (OR 0.68/SOFA point, 95% CI 0.52 to 0.88), bacterial infection (OR 0.43, 95% CI 0.21 to 0.90), three or four quadrants involved on chest X-ray (OR 0.44, 95% CI 0.21 to 0.91), time from hospital to ICU admission (OR 0.98/day, 95% CI 0.95 to 0.99) and oxygen flow at admission (OR 0.93/liter, 95% CI 0.86 to 0.99).
Conclusions: In kidney transplant recipients, ARF is associated with high mortality and graft loss rates. Increased Pneumocystis and bacterial prophylaxis might improve these outcomes. Early ICU admission might prevent graft loss.
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725–1730. doi: 10.1056/NEJM199912023412303. - DOI - PubMed
-
- Kamar N, Garrigue V, Karras A, Mourad G, Lefrançois N, Charpentier B, Legendre C, Rostaing L. Impact of early or delayed cyclosporine on delayed graft function in renal transplant recipients: a randomized, multicenter study. Am J Transplant. 2006;6:1042–1048. doi: 10.1111/j.1600-6143.2006.01291.x. - DOI - PubMed
-
- Mourad G, Karras A, Kamar N, Garrigue V, Legendre C, Lefrançois N, Charpentier B, Bourbigot B, Pouteil-Nobil C, Bayle F, Lebranchu Y, Mariat C, Le Meur Y, Kessler M, Moulin B, Ducloux D, Delahousse M, Lang P, Merville P, Chaouche-Teyara K, Rostaing L. French Myriade FR01 Study Group. Renal function with delayed or immediate cyclosporine microemulsion in combination with enteric-coated mycophenolate sodium and steroids: results of follow up to 30 months post-transplant. Clin Transplant. 2007;21:295–300. doi: 10.1111/j.1399-0012.2007.00660.x. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
