

Use of weekly, low dose, high frequency ultrasound for hard to heal venous leg ulcers: the VenUS III randomised controlled trial
- PMID: 21385806
- PMCID: PMC3050437
- DOI: 10.1136/bmj.d1092
Use of weekly, low dose, high frequency ultrasound for hard to heal venous leg ulcers: the VenUS III randomised controlled trial
Abstract
Objective: To assess the clinical effectiveness of weekly delivery of low dose, high frequency therapeutic ultrasound in conjunction with standard care for hard to heal venous leg ulcers.
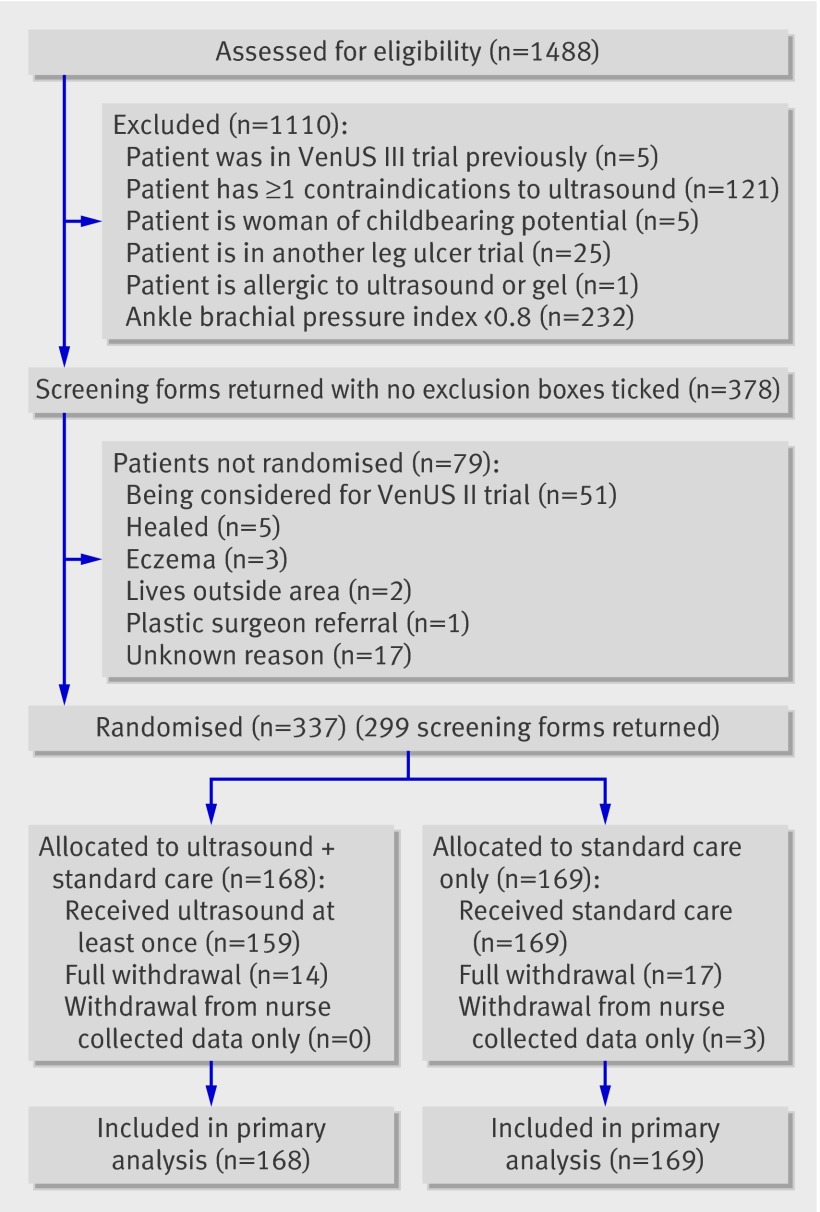
Design: Multicentre, pragmatic, two arm randomised controlled trial.
Setting: Community and district nurse led services, community leg ulcer clinics, and hospital outpatient leg ulcer clinics in 12 urban and rural settings (11 in the United Kingdom and one in the Republic of Ireland).
Participants: 337 patients with at least one venous leg ulcer of >6 months' duration or >5 cm(2) area and an ankle brachial pressure index of ≥ 0.8.
Interventions: Weekly administration of low dose, high frequency ultrasound therapy (0.5 W/cm(2), 1 MHz, pulsed pattern of 1:4) for up to 12 weeks plus standard care compared with standard care alone.
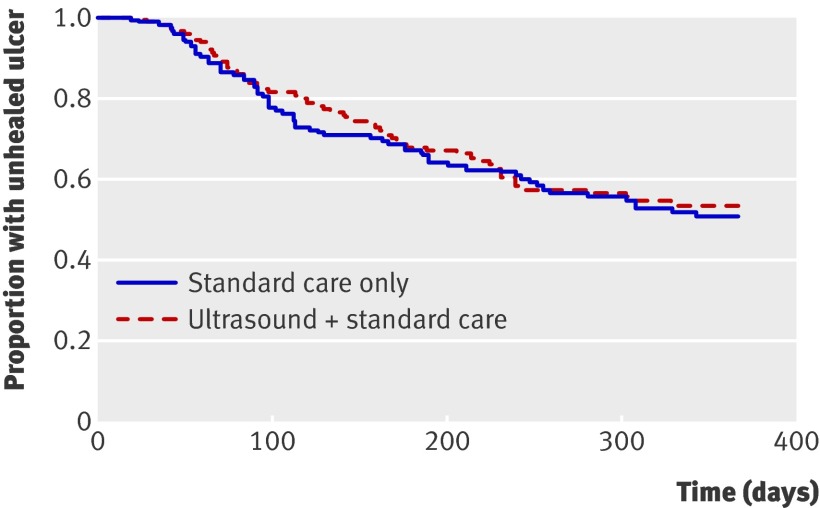
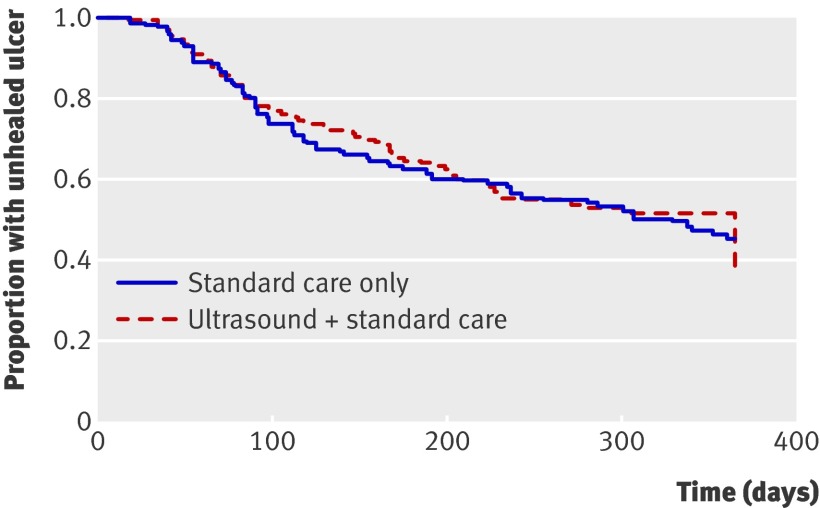
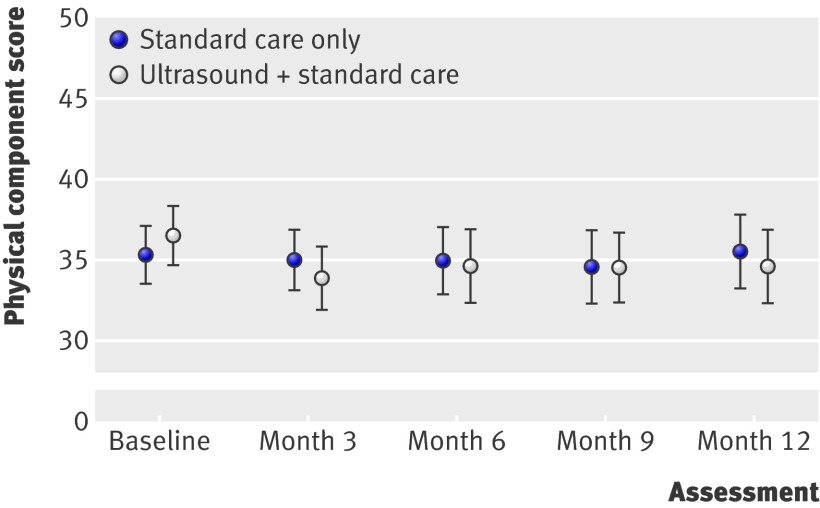
Main outcome measures: Primary outcome was time to healing of the largest eligible leg ulcer. Secondary outcomes were proportion of patients healed by 12 months, percentage and absolute change in ulcer size, proportion of time participants were ulcer-free, health related quality of life, and adverse events.
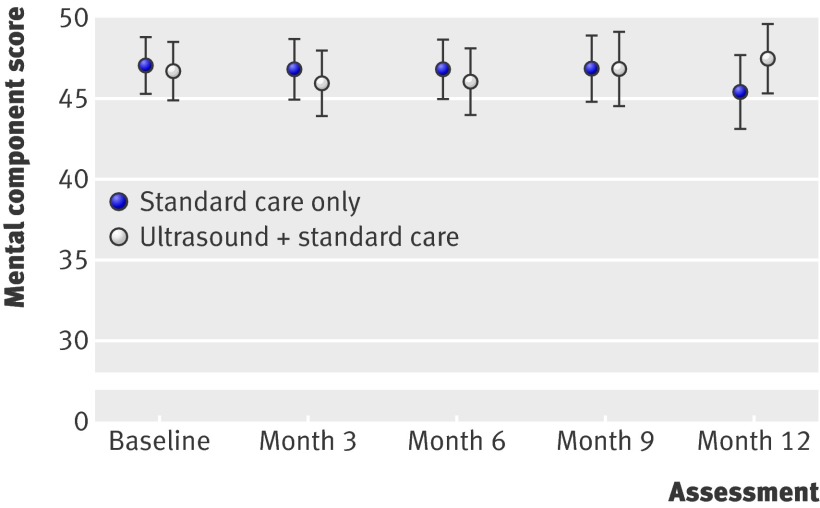
Results: The two groups showed no significant difference in the time to healing of the reference leg ulcer (log rank test, P=0.61). After adjustment for baseline ulcer area, baseline ulcer duration, use of compression bandaging, and study centre, there was still no evidence of a difference in time to healing (hazard ratio 0.99 (95% confidence interval 0.70 to 1.40), P=0.97). The median time to healing of the reference leg ulcer was inestimable. There was no significant difference between groups in the proportion of participants with all ulcers healed by 12 months (72/168 in ultrasound group v 78/169 in standard care group, P=0.39 for Fisher's exact test) nor in the change in ulcer size at four weeks by treatment group (model estimate 0.05 (95% CI -0.09 to 0.19)). There was no difference in time to complete healing of all ulcers (log rank test, P=0.61), with median time to healing of 328 days (95% CI 235 to inestimable) with standard care and 365 days (224 days to inestimable) with ultrasound. There was no evidence of a difference in rates of recurrence of healed ulcers (17/31 with ultrasound v 14/31 with standard care, P=0.68 for Fisher's exact test). There was no difference between the two groups in health related quality of life, both for the physical component score (model estimate 0.69 (-1.79 to 3.08)) and the mental component score (model estimate -0.93 (-3.30 to 1.44)), but there were significantly more adverse events in the ultrasound group (model estimate 0.30 (0.01 to 0.60)). There was a significant relation between time to ulcer healing and baseline ulcer area (hazard ratio 0.64 (0.55 to 0.75)) and baseline ulcer duration (hazard ratio 0.59 (0.50 to 0.71)), with larger and older ulcers taking longer to heal. In addition, those centres with high recruitment rates had the highest healing rates.
Conclusions: Low dose, high frequency ultrasound administered weekly for 12 weeks during dressing changes in addition to standard care did not increase ulcer healing rates, affect quality of life, or reduce ulcer recurrence. Trial registration ISRCTN21175670 and National Research Register N0484162339.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Graham ID, Harrison MB, Nelson EA, Lorimer K, Fisher A. Prevalence of lower-limb ulceration: a systematic review of prevalence studies. Adv Skin Wound Care 2003;16:305-16. - PubMed
-
- Dale JJ, Callam MJ, Ruckley CV, Harper DR, Berrey PN. Chronic ulcers of the leg: a study of prevalence in a Scottish community. Health Bulletin (Edin) 1983;41:311-4. - PubMed
-
- Briggs M, Flemming K. Living with leg ulceration: a synthesis of qualitative research. J Adv Nurs 2007;59:319-28. - PubMed
-
- O’Meara S, Cullum NA, Nelson EA. Compression for venous leg ulcers. Cochrane Database Syst Rev 2008;4:CD000265. - PubMed
-
- Iglesias C, Nelson EA, Cullum NA, Torgerson DJ, for the VenUS Team. The VenUS I Trial: a randomised comparison of 4-layer and short-stretch bandages for the treatment of venous leg ulcers. Health Technol Assess 2004;8:iii,1-105. - PubMed