

Age-related EBV-associated lymphoproliferative disorders in the Western population: a spectrum of reactive lymphoid hyperplasia and lymphoma
- PMID: 21385849
- PMCID: PMC3100685
- DOI: 10.1182/blood-2010-12-323238
Age-related EBV-associated lymphoproliferative disorders in the Western population: a spectrum of reactive lymphoid hyperplasia and lymphoma
Abstract
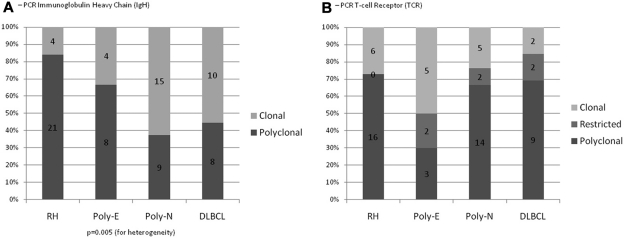
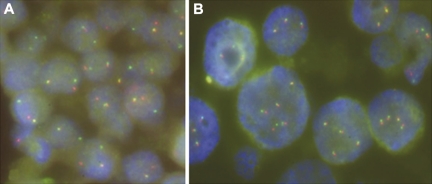
We investigated age-related EBV(+) B-cell lymphoproliferations in the Western population. The clinical features, histology, immunophenotype, EBV-encoded RNA in situ hybridization, and clonality by PCR of T-cell receptor gamma and immunoglobulin genes were categorized in 122 EBV(+) lesions as follows: (1) reactive lymphoid hyperplasia; (2) polymorphic extranodal or (3) polymorphic nodal lymphoproliferative disease (LPD); and (4) diffuse large B-cell lymphoma (DLBCL). Interphase FISH for IG and PAX5 gene rearrangements was performed on 17 cases of DLBCL. The overall median age was 75 years (range, 45-101 years; 67 men, 55 women), and 67, 79, 73, and 77 years, respectively, for groups 1 through 4. Sixteen of 21 cases of polymorphic extranodal LPD were classified as EBV(+) mucocutaneous ulcer. PCR for immunoglobulin genes was polyclonal in reactive lymphoid hyperplasia (84%) and monoclonal in 33%, 63%, and 56% of polymorphic extranodal and nodal LPD cases and DLBCL, respectively. All groups showed restricted/clonal T-cell receptor responses (27%-70%). By FISH, 19% of DLBCLs showed IGH@ rearrangements, but PAX5 was unaffected. Disease-specific 5-year survival was 100%, 93%, 57%, and 25% for groups 1-4, respectively, and 100% for patients with EBV(+) mucocutaneous ulcer. Disease volume was predictive of therapy response (P = .0002), and pathologic subtype was predictive of overall outcome (P = .001). Age-related EBV(+) B-cell LPD encompasses a wider disease spectrum than previously recognized and includes both reactive and neoplastic conditions. Reduction in the T-cell repertoire may contribute to decreased immune surveillance.
Figures



References
-
- Hislop AD, Taylor GS, Sauce D, Rickinson AB. Cellular responses to viral infection in humans: lessons from Epstein-Barr virus. Annu Rev Immunol. 2007;25:587–617. - PubMed
-
- Klein E, Kis LL, Klein G. Epstein-Barr virus infection in humans: from harmless to life endangering virus-lymphocyte interactions. Oncogene. 2007;26(9):1297–1305. - PubMed
-
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue. 4th ed. Lyon, France: IARC; 2008.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
