

Conductive keratoplasty for the treatment of presbyopia: comparative study between post- and non-LASIK eyes
- PMID: 21386916
- PMCID: PMC3046993
- DOI: 10.2147/OPTH.S16791
Conductive keratoplasty for the treatment of presbyopia: comparative study between post- and non-LASIK eyes
Abstract
Purpose: To evaluate the efficacy and safety of conductive keratoplasty (CK) for the treatment of presbyopia and analyze the differences in the effects between post- and non-laser in situ keratomileusis (LASIK) eyes. Clinical preoperative factors that could affect the predictability of CK were also analyzed.
Methods: The visual and refractive outcomes of CK for the treatment of presbyopia in 14 eyes of 13 post-LASIK patients (post-LASIK group mean age 50.9 ± 3.4 years) and those of 25 eyes of 25 non-LASIK patients (non-LASIK group mean age 52.4 ± 4.0 years) were studied. The clinical efficacy, safety, stability, and predictability of CK were statistically evaluated.
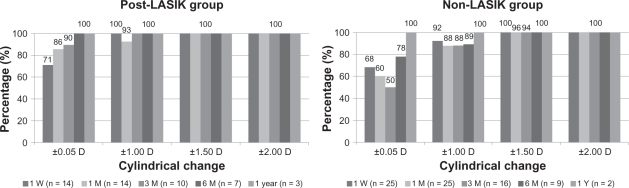
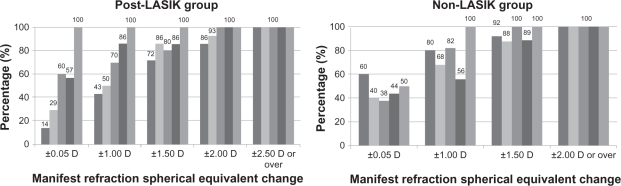
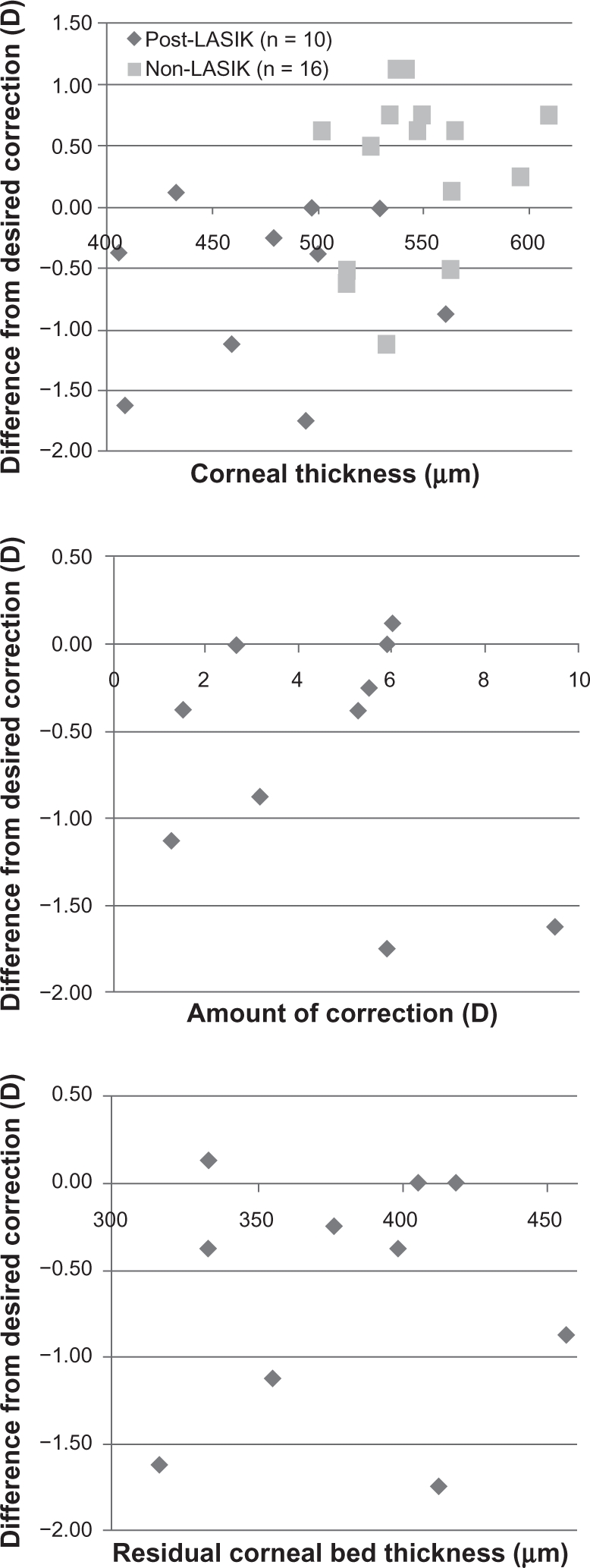
Results: The mean (logarithm of the minimum angle of resolution [logMAR] ± standard deviation [SD]) of preoperative uncorrected near visual acuity (UNVA) and manifest refraction spherical equivalent (MRSE) were 0.64 ± 0.25 diopter (D) and 0.35 ± 0.48 D, respectively, in the post-LASIK group, and 0.71 ± 0.20 D and 0.64 ± 0.61 D, respectively, in the non-LASIK group. At 6 months after CK, the mean UNVA and MRSE were 0.07 ± 0.13 D and -1.59 ± 0.86 D, respectively, in the post-LASIK group, and 0.07 ± 0.12 D and -1.06 ± 0.56 D, respectively, in the non-LASIK group. At 1 year after CK, the mean UNVA and MRSE were 0.30 ± 0.17 D and -0.58 ± 0.52 D, respectively, in the post-LASIK group, and 0.28 ± 0.34 D and -1.56 ± 0.62 D, respectively, in the non-LASIK group. There was no significant difference between the two groups in either factor at 6 months postoperative (Student's t-test, P > 0.05). At 1 year after CK, all the treated eyes maintained corrected distance visual acuity better than -0.08 (logMAR). The mean cylindrical errors were within ±1.00 D in 100% of the post-LASIK and non-LASIK patients. As for the preoperative clinical factors evaluated for their potential relationship to the predictability of CK, none showed significant effect on the clinical outcomes.
Conclusion: CK is demonstrated to be safe for the treatment of presbyopia in post-LASIK patients as well as in non-LASIK patients, though needed longer observation in terms of factors affecting predictability.
Keywords: CK; conductive keratoplasty; post-LASIK; presbyopia.
Figures
Similar articles
-
Comparing the rate of regression after conductive keratoplasty with or without prior laser-assisted in situ keratomileusis or photorefractive keratectomy.Middle East Afr J Ophthalmol. 2012 Oct;19(4):377-81. doi: 10.4103/0974-9233.102743. Middle East Afr J Ophthalmol. 2012. PMID: 23248539 Free PMC article.
-
Five-Year Results of Combined Small-Aperture Corneal Inlay Implantation and LASIK for the Treatment of Hyperopic Presbyopic Eyes.J Refract Surg. 2020 Aug 1;36(8):498-505. doi: 10.3928/1081597X-20200618-01. J Refract Surg. 2020. PMID: 32785722
-
Safety and effectiveness of the SUPRACOR presbyopic LASIK algorithm on hyperopic patients.Eye Vis (Lond). 2016 Dec 8;3:33. doi: 10.1186/s40662-016-0062-6. eCollection 2016. Eye Vis (Lond). 2016. PMID: 27981059 Free PMC article.
-
Outcomes of presbyopia-correcting intraocular lenses after laser in situ keratomileusis.Int Ophthalmol. 2019 May;39(5):1199-1204. doi: 10.1007/s10792-018-0908-0. Epub 2018 Mar 28. Int Ophthalmol. 2019. PMID: 29594789 Review.
-
Efficacy, Safety, Predictability, and Stability of LASIK for Presbyopia Correction: A Systematic Review and Meta-analysis.J Refract Surg. 2023 Sep;39(9):627-638. doi: 10.3928/1081597X-20230802-02. Epub 2023 Sep 1. J Refract Surg. 2023. PMID: 37675909
Cited by
-
Comparing the rate of regression after conductive keratoplasty with or without prior laser-assisted in situ keratomileusis or photorefractive keratectomy.Middle East Afr J Ophthalmol. 2012 Oct;19(4):377-81. doi: 10.4103/0974-9233.102743. Middle East Afr J Ophthalmol. 2012. PMID: 23248539 Free PMC article.
-
[Evaluation and quality assurance of refractive surgery procedures by the German Ophthalmological Society and the Professional Association of German Ophthalmologists. Status: May 2011].Ophthalmologe. 2011 Sep;108(9):869-82. doi: 10.1007/s00347-011-2415-9. Ophthalmologe. 2011. PMID: 21909873 German.
-
Corneal Refractive Procedures for the Treatment of Presbyopia.Open Ophthalmol J. 2017 Apr 27;11:59-75. doi: 10.2174/1874364101711010059. eCollection 2017. Open Ophthalmol J. 2017. PMID: 28553423 Free PMC article. Review.
-
Updates on Managements for Keratoconus.J Curr Ophthalmol. 2017 Dec 6;30(2):110-124. doi: 10.1016/j.joco.2017.11.002. eCollection 2018 Jun. J Curr Ophthalmol. 2017. PMID: 29988906 Free PMC article. Review.
References
-
- Guputa N, Naroo SA, Wolffsohn S. Visual comparison of multifocal lens to monovision. Optom Vis Sci. 2009;86:E98–E105. - PubMed
-
- Reilly CD, Lee WB, Alvarenga L, et al. Surgical monovision and monovision reversal in LASIK. Cornea. 2006;25:136–138. - PubMed
-
- Braun EHP, Lee J, Steinert RF. Monovision in LASIK. Ophthalmology. 2008;115:1196–1202. - PubMed
-
- Telandro A. The pseudoaccommodative cornea multifocal ablation with a center-distance pattern: a Review. J Refract Surg. 2009;25(Suppl):S156–S159. - PubMed
-
- El Danasoury AM, Gamaly TO, Hantera M. Multizone. LASIK with peripheral near zone for correction of presbyopia in myopic and hyperopic eyes: 1-year results. J Refract Surg. 2009;25:296–305. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
