

Medication adherence among community-dwelling patients with heart failure
- PMID: 21389248
- PMCID: PMC3068886
- DOI: 10.4065/mcp.2010.0732
Medication adherence among community-dwelling patients with heart failure
Abstract
Objective: To determine medication use and adherence among community-dwelling patients with heart failure (HF).
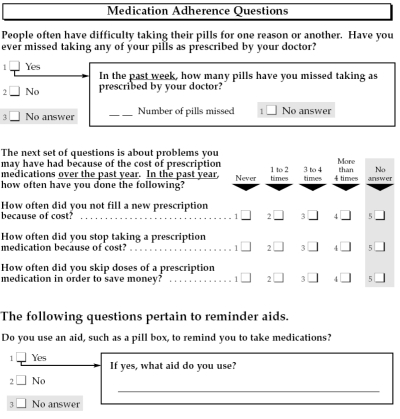
Patients and methods: Residents of Olmsted County, Minnesota, with HF were recruited from October 10, 2007, through February 25, 2009. Pharmacy records were obtained for the 6 months after enrollment. Medication adherence was measured by the proportion of days covered (PDC). A PDC of less than 80% was classified as poor adherence. Factors associated with medication adherence were investigated.
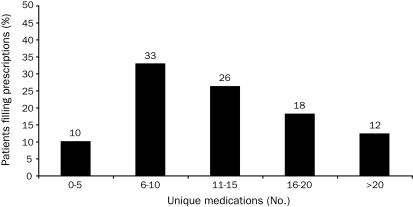
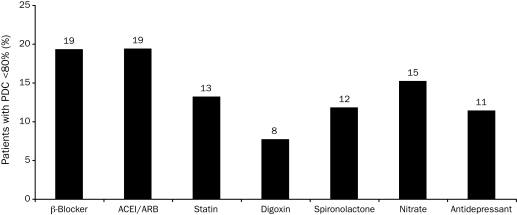
Results: Among the 209 study patients with HF, 123 (59%) were male, and the mean ± SD age was 73.7 ± 13.5 years. The median (interquartile range) number of unique medications filled during the 6-month study period was 11 (8-17). Patients with a documented medication allergy were excluded from eligibility for medication use within that medication class. Most patients received conventional HF therapy: 70% (147/209) were treated with β-blockers and 75% (149/200) with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers. Most patients (62%; 127/205) also took statins. After exclusion of patients with missing dosage information, the proportion of those with poor adherence was 19% (27/140), 19% (28/144), and 13% (16/121) for β-blockers, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, and statins, respectively. Self-reported data indicated that those with poor adherence experienced more cost-related medication issues. For example, those who adhered poorly to statin therapy more frequently reported stopping a prescription because of cost than those with good adherence (46% vs 6%; P < .001), skipping doses to save money (23% vs 3%; P = .03), and not filling a new prescription because of cost (46% vs 6%; P < .001).
Conclusion: Community-dwelling patients with HF take a large number of medications. Medication adherence was suboptimal in many patients, often because of cost.
Figures
Comment in
-
Medication adherence: hope for improvement?Mayo Clin Proc. 2011 Apr;86(4):268-70. doi: 10.4065/mcp.2011.0123. Mayo Clin Proc. 2011. PMID: 21454729 Free PMC article. No abstract available.
References
-
- Writing Group Members Heart disease and stroke statistics–2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee [published corrections appear in Circulation. 2010;122 (1):ell and 2009;119(3):e182] Circulation. 2009;119(3):e21-e181 - PubMed
-
- Writing Committee Members. Task Force Members ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). Circulation. 2005;112(12):e154-e235 - PubMed
-
- Murray MD, Young J, Hoke S, et al. Pharmacist intervention to improve medication adherence in heart failure: a randomized trial. Ann Intern Med. 2007;146(10):714-725 - PubMed
-
- Bagchi AD, Esposito D, Kim M, Verdier J, Bencio D. Utilization of, and adherence to, drug therapy among medicaid beneficiaries with congestive heart failure. Clin Ther. 2007;29(8):1771-1783 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
