

Single center experience of capsule endoscopy in patients with obscure gastrointestinal bleeding
- PMID: 21390148
- PMCID: PMC3042656
- DOI: 10.3748/wjg.v17.i6.774
Single center experience of capsule endoscopy in patients with obscure gastrointestinal bleeding
Abstract
Aim: To identify optimum timing to maximize diagnostic yield by capsule endoscopy (CE) in patients with obscure gastrointestinal bleeding (OGIB).
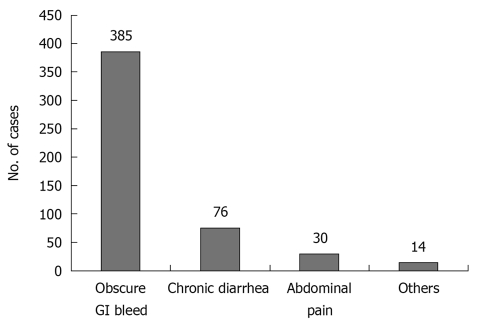
Methods: We identified patients who underwent CE at our institution from August 2003 to December 2009. Patient medical records were reviewed to determine type of OGIB (occult, overt), CE results and complications, and timing of CE with respect to onset of bleeding.
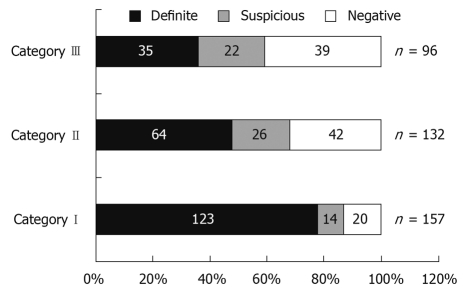
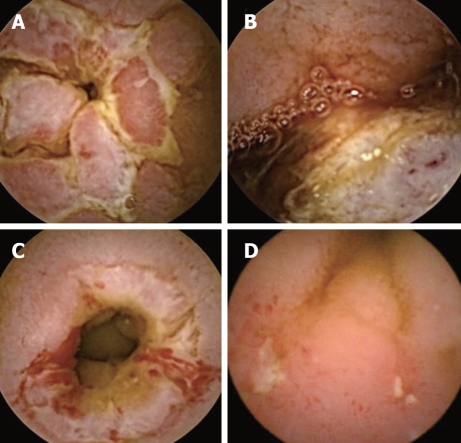
Results: Out of 385 patients investigated for OGIB, 284 (74%) had some lesion detected by CE. In 222 patients (58%), definite lesions were detected that could unequivocally explain OGIB. Small bowel ulcer/erosions secondary to Crohn's disease, tuberculosis or non-steroidal anti-inflammatory agent use were the commonest lesions detected. Patients with overt GI bleeding for < 48 h before CE had the highest diagnostic yield (87%). This was significantly greater (P < 0.05) compared to that in patients with overt bleeding prior to 48 h (68%), as well as those with occult OGIB (59%).
Conclusion: We established the importance of early CE in management of OGIB. CE within 48 h of overt bleeding has the greatest potential for lesion detection.
Keywords: Capsule endoscopy; Gastrointestinal bleeding.
Figures
References
-
- Cellier C. Obscure gastrointestinal bleeding: role of videocapsule and double-balloon enteroscopy. Best Pract Res Clin Gastroenterol. 2008;22:329–340. - PubMed
-
- Ell C, Remke S, May A, Helou L, Henrich R, Mayer G. The first prospective controlled trial comparing wireless capsule endoscopy with push enteroscopy in chronic gastrointestinal bleeding. Endoscopy. 2002;34:685–689. - PubMed
-
- Lim RM, O’Loughlin CJ, Barkin JS. Comparison of wireless capsule endoscopy (M2A™) with push enteroscopy in the evaluation of obscure gastrointestinal bleeding. Am J Gastroenterol. 2002;97:S83.
-
- Costamagna G, Shah SK, Riccioni ME, Foschia F, Mutignani M, Perri V, Vecchioli A, Brizi MG, Picciocchi A, Marano P. A prospective trial comparing small bowel radiographs and video capsule endoscopy for suspected small bowel disease. Gastroenterology. 2002;123:999–1005. - PubMed
-
- Hara AK, Leighton JA, Sharma VK, Fleischer DE. Small bowel: preliminary comparison of capsule endoscopy with barium study and CT. Radiology. 2004;230:260–265. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
