

A randomized controlled trial comparing the effects of counseling and alarm device on HAART adherence and virologic outcomes
- PMID: 21390262
- PMCID: PMC3046986
- DOI: 10.1371/journal.pmed.1000422
A randomized controlled trial comparing the effects of counseling and alarm device on HAART adherence and virologic outcomes
Abstract
Background: Behavioral interventions that promote adherence to antiretroviral medications may decrease HIV treatment failure. Antiretroviral treatment programs in sub-Saharan Africa confront increasing financial constraints to provide comprehensive HIV care, which include adherence interventions. This study compared the impact of counseling and use of an alarm device on adherence and biological outcomes in a resource-limited setting.
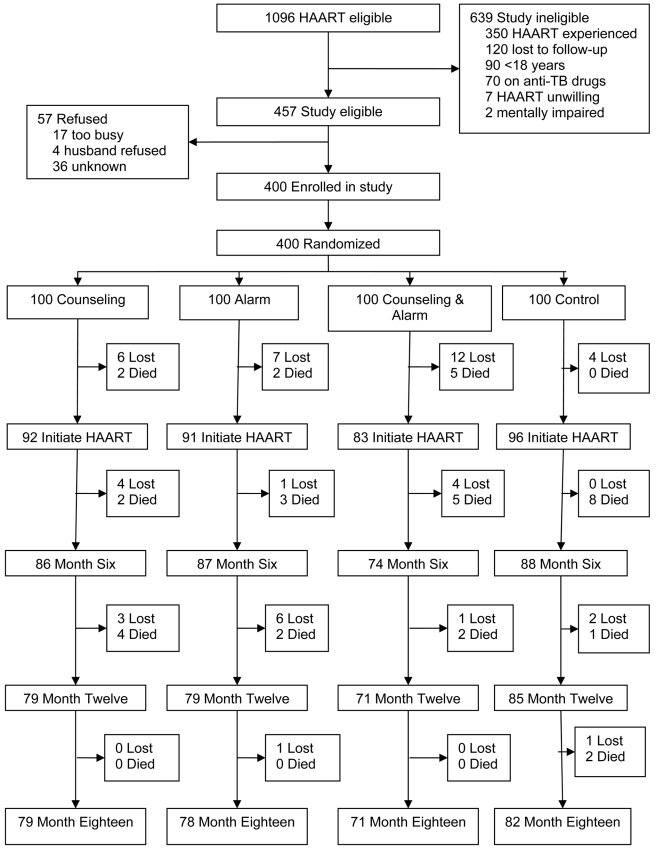
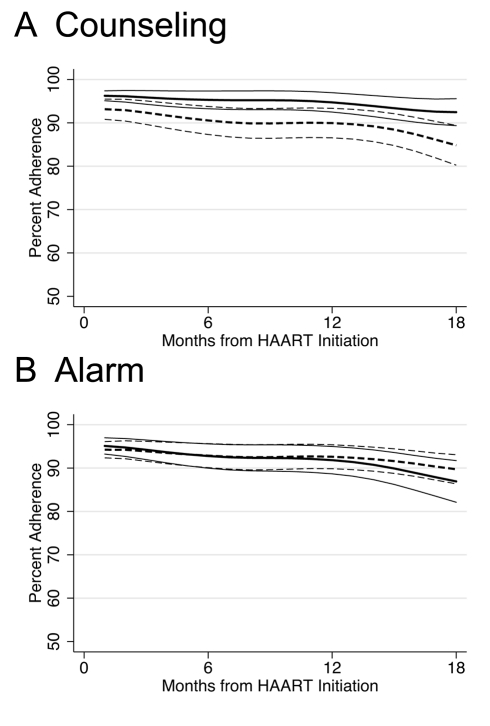
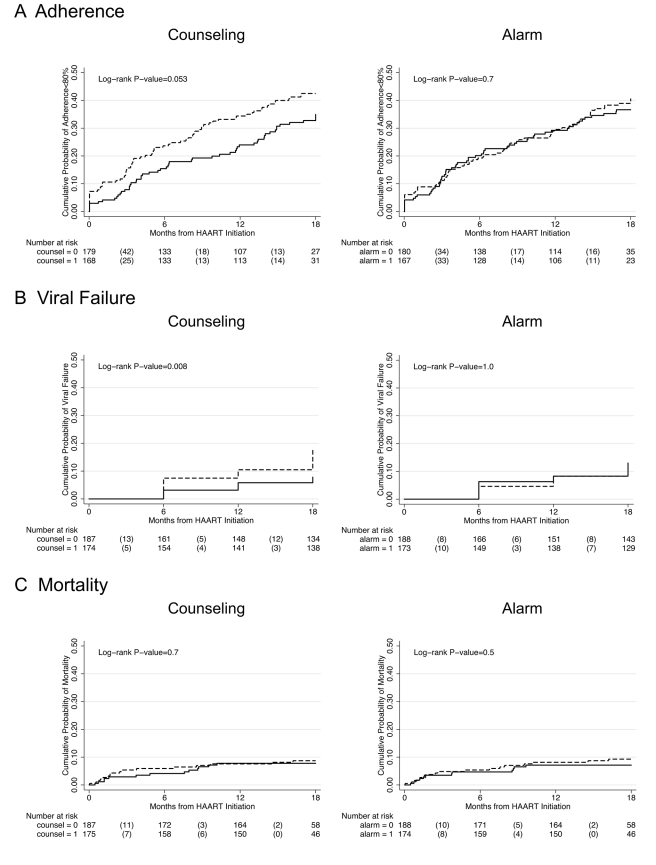
Methods and findings: A randomized controlled, factorial designed trial was conducted in Nairobi, Kenya. Antiretroviral-naïve individuals initiating free highly active antiretroviral therapy (HAART) in the form of fixed-dose combination pills (d4T, 3TC, and nevirapine) were randomized to one of four arms: counseling (three counseling sessions around HAART initiation), alarm (pocket electronic pill reminder carried for 6 months), counseling plus alarm, and neither counseling nor alarm. Participants were followed for 18 months after HAART initiation. Primary study endpoints included plasma HIV-1 RNA and CD4 count every 6 months, mortality, and adherence measured by monthly pill count. Between May 2006 and September 2008, 400 individuals were enrolled, 362 initiated HAART, and 310 completed follow-up. Participants who received counseling were 29% less likely to have monthly adherence <80% (hazard ratio [HR] = 0.71; 95% confidence interval [CI] 0.49-1.01; p = 0.055) and 59% less likely to experience viral failure (HIV-1 RNA ≥5,000 copies/ml) (HR 0.41; 95% CI 0.21-0.81; p = 0.01) compared to those who received no counseling. There was no significant impact of using an alarm on poor adherence (HR 0.93; 95% CI 0.65-1.32; p = 0.7) or viral failure (HR 0.99; 95% CI 0.53-1.84; p = 1.0) compared to those who did not use an alarm. Neither counseling nor alarm was significantly associated with mortality or rate of immune reconstitution.
Conclusions: Intensive early adherence counseling at HAART initiation resulted in sustained, significant impact on adherence and virologic treatment failure during 18-month follow-up, while use of an alarm device had no effect. As antiretroviral treatment clinics expand to meet an increasing demand for HIV care in sub-Saharan Africa, adherence counseling should be implemented to decrease the development of treatment failure and spread of resistant HIV.
Trial registration: ClinicalTrials.gov NCT00273780.
Conflict of interest statement
Academic Editor Edward Mills has collaborated and published one previous paper with Michael Chung, the lead author on this paper.
Figures
References
-
- Harries AD, Nyangulu DS, Hargreaves NJ, Kaluwa O, Salaniponi FM. Preventing antiretroviral anarchy in sub-Saharan Africa. Lancet. 2001;358:410–414. - PubMed
-
- Orrell C, Bangsberg DR, Badri M, Wood R. Adherence is not a barrier to successful antiretroviral therapy in South Africa. AIDS. 2003;17:1369–1375. - PubMed
-
- Mills EJ, Nachega JB, Buchan I, Orbinski J, Attaran A, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: a meta-analysis. JAMA. 2006;296:679–690. - PubMed
-
- Calmy A, Pinoges L, Szumilin E, Zachariah R, Ford N, et al. Generic fixed-dose combination antiretroviral treatment in resource-poor settings: multicentric observational cohort. AIDS. 2006;20:1163–1169. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
