

Informed switching strongly decreases the prevalence of antibiotic resistance in hospital wards
- PMID: 21390265
- PMCID: PMC3048378
- DOI: 10.1371/journal.pcbi.1001094
Informed switching strongly decreases the prevalence of antibiotic resistance in hospital wards
Abstract
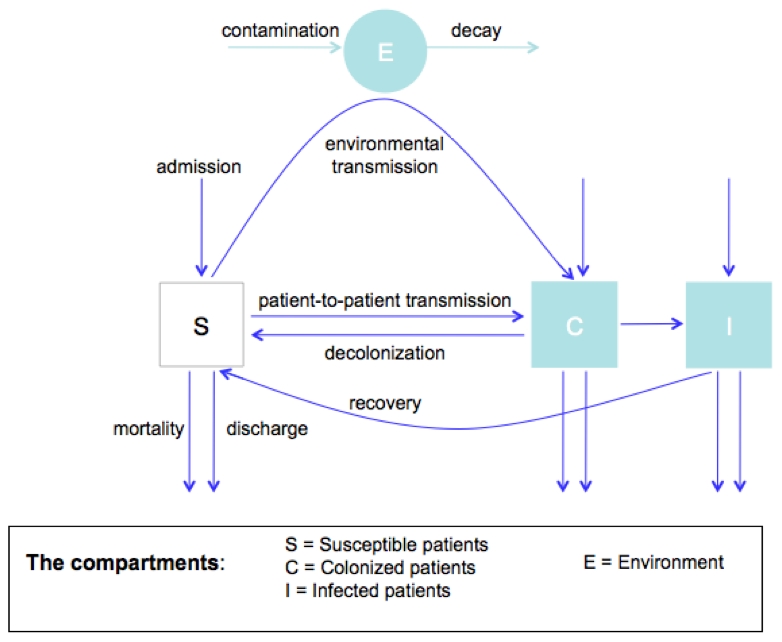
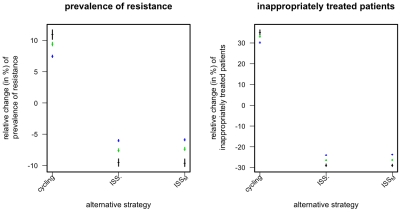
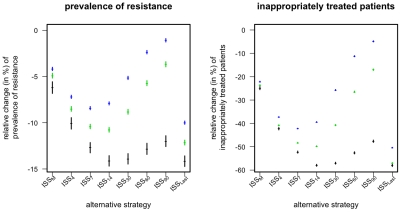
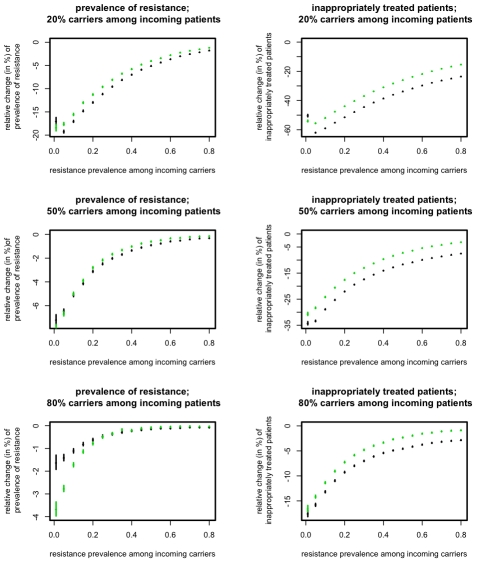
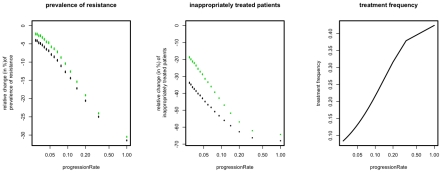
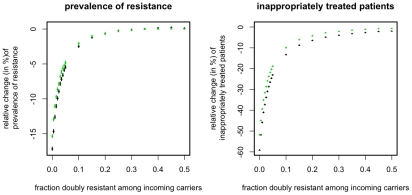
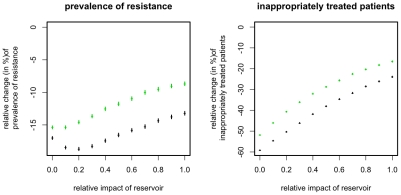
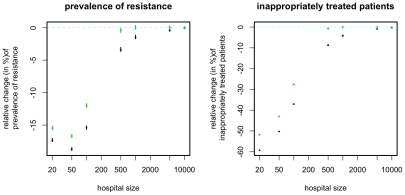
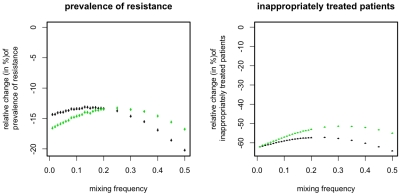
Antibiotic resistant nosocomial infections are an important cause of mortality and morbidity in hospitals. Antibiotic cycling has been proposed to contain this spread by a coordinated use of different antibiotics. Theoretical work, however, suggests that often the random deployment of drugs ("mixing") might be the better strategy. We use an epidemiological model for a single hospital ward in order to assess the performance of cycling strategies which take into account the frequency of antibiotic resistance in the hospital ward. We assume that information on resistance frequencies stems from microbiological tests, which are performed in order to optimize individual therapy. Thus the strategy proposed here represents an optimization at population-level, which comes as a free byproduct of optimizing treatment at the individual level. We find that in most cases such an informed switching strategy outperforms both periodic cycling and mixing, despite the fact that information on the frequency of resistance is derived only from a small sub-population of patients. Furthermore we show that the success of this strategy is essentially a stochastic phenomenon taking advantage of the small population sizes in hospital wards. We find that the performance of an informed switching strategy can be improved substantially if information on resistance tests is integrated over a period of one to two weeks. Finally we argue that our findings are robust against a (moderate) preexistence of doubly resistant strains and against transmission via environmental reservoirs. Overall, our results suggest that switching between different antibiotics might be a valuable strategy in small patient populations, if the switching strategies take the frequencies of resistance alleles into account.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Antibiotic control of antibiotic resistance in hospitals: a simulation study.BMC Infect Dis. 2010 Aug 25;10:254. doi: 10.1186/1471-2334-10-254. BMC Infect Dis. 2010. PMID: 20738872 Free PMC article.
-
Cycling empirical antibiotic therapy in hospitals: meta-analysis and models.PLoS Pathog. 2014 Jun 26;10(6):e1004225. doi: 10.1371/journal.ppat.1004225. eCollection 2014 Jun. PLoS Pathog. 2014. PMID: 24968123 Free PMC article.
-
Metapopulation ecology links antibiotic resistance, consumption, and patient transfers in a network of hospital wards.Elife. 2020 Oct 27;9:e54795. doi: 10.7554/eLife.54795. Elife. 2020. PMID: 33106223 Free PMC article.
-
Clinical significance of the emergence of bacterial resistance in the hospital environment.J Appl Microbiol. 2002;92 Suppl:90S-7S. J Appl Microbiol. 2002. PMID: 12000618 Review.
-
Antibiotic resistance in hospital pathogens--acquisition or spread?Int J Antimicrob Agents. 2001 Sep;18(3):295-8. doi: 10.1016/s0924-8579(01)00378-8. Int J Antimicrob Agents. 2001. PMID: 11673047 Review.
Cited by
-
Population-level mathematical modeling of antimicrobial resistance: a systematic review.BMC Med. 2019 Apr 24;17(1):81. doi: 10.1186/s12916-019-1314-9. BMC Med. 2019. PMID: 31014341 Free PMC article.
-
Modelling the transmission of healthcare associated infections: a systematic review.BMC Infect Dis. 2013 Jun 28;13:294. doi: 10.1186/1471-2334-13-294. BMC Infect Dis. 2013. PMID: 23809195 Free PMC article.
-
The effects of antibiotic cycling and mixing on acquisition of antibiotic resistant bacteria in the ICU: A post-hoc individual patient analysis of a prospective cluster-randomized crossover study.PLoS One. 2022 May 3;17(5):e0265720. doi: 10.1371/journal.pone.0265720. eCollection 2022. PLoS One. 2022. PMID: 35503768 Free PMC article. Clinical Trial.
-
Evolutionary epidemiology models to predict the dynamics of antibiotic resistance.Evol Appl. 2019 Jan 21;12(3):365-383. doi: 10.1111/eva.12753. eCollection 2019 Mar. Evol Appl. 2019. PMID: 30828361 Free PMC article.
-
A data-driven mathematical model of multi-drug resistant Acinetobacter baumannii transmission in an intensive care unit.Sci Rep. 2015 Mar 25;5:9478. doi: 10.1038/srep09478. Sci Rep. 2015. PMID: 25804674 Free PMC article.
References
-
- Niederman MS. Impact of antibiotic resistance on clinical outcomes and the cost of care. Crit Care Med. 2001;29:N114–120. - PubMed
-
- Brown EM, Nathwani D. Antibiotic cycling or rotation: a systematic review of the evidence of efficacy. J Antimicrob Chemother. 2005;55:6–9. - PubMed
-
- Masterton RG. Antibiotic cycling: more than it might seem? J Antimicrob Chemother. 2005;55:1–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
