

Chronic ankle instability: evolution of the model
- PMID: 21391798
- PMCID: PMC3070500
- DOI: 10.4085/1062-6050-46.2.133
Chronic ankle instability: evolution of the model
Abstract
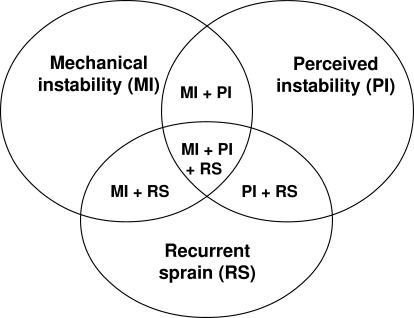
Context: The Hertel model of chronic ankle instability (CAI) is commonly used in research but may not be sufficiently comprehensive. Mechanical instability and functional instability are considered part of a continuum, and recurrent sprain occurs when both conditions are present. A modification of the Hertel model is proposed whereby these 3 components can exist independently or in combination.
Objective: To examine the fit of data from people with CAI to 2 CAI models and to explore whether the different subgroups display impairments when compared with a control group.
Design: Cross-sectional study.
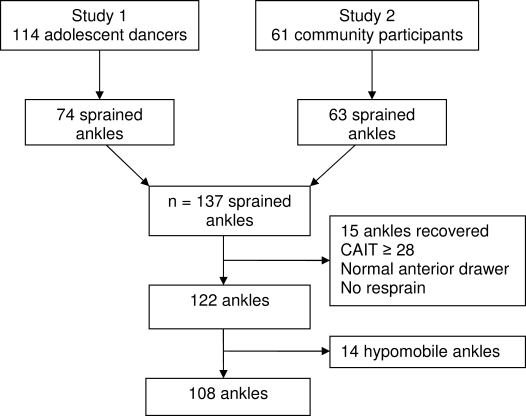
Patients or other participants: Community-dwelling adults and adolescent dancers were recruited: 137 ankles with ankle sprain for objective 1 and 81 with CAI and 43 controls for objective 2.
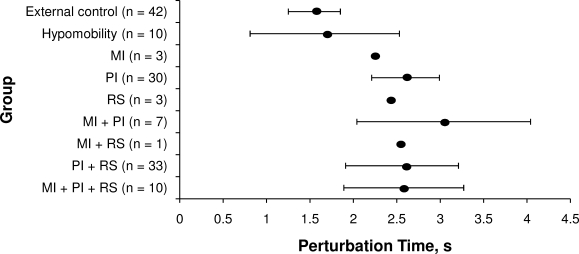
Intervention(s): Two balance tasks and time to recover from an inversion perturbation were assessed to determine if the subgroups demonstrated impairments when compared with a control group (objective 2).
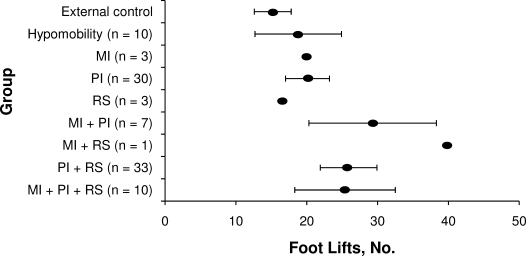
Main outcome measure(s): For objective 1 (fit to the 2 models), outcomes were Cumberland Ankle Instability Tool score, anterior drawer test results, and number of sprains. For objective 2, outcomes were 2 balance tasks (number of foot lifts in 30 seconds, ability to balance on the ball of the foot) and time to recover from an inversion perturbation. The Cohen d was calculated to compare each subgroup with the control group.
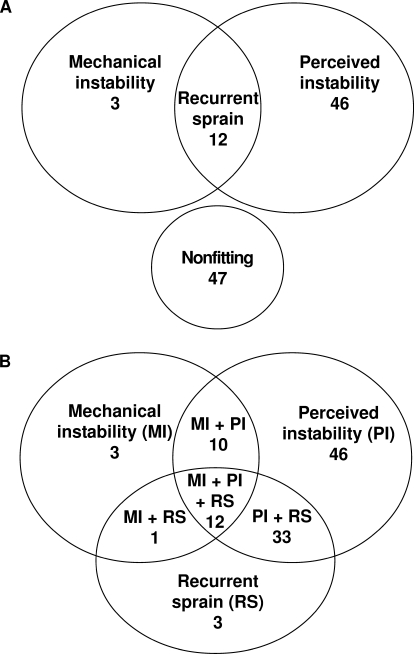
Results: A total of 56.5% of ankles (n = 61) fit the Hertel model, whereas all ankles (n = 108) fit the proposed model. In the proposed model, 42.6% of ankles were classified as perceived instability, 30.5% as recurrent sprain and perceived instability, and 26.9% as among the remaining groups. All CAI subgroups performed more poorly on the balance and inversion-perturbation tasks than the control group. Subgroups with perceived instability had greater impairment in single-leg stance, whereas participants with recurrent sprain performed more poorly than the other subgroups when balancing on the ball of the foot. Only individuals with hypomobility appeared unimpaired when recovering from an inversion perturbation.
Conclusions: The new model of CAI is supported by the available data. Perceived instability alone and in combination characterized the majority of participants. Several impairments distinguished the sprain groups from the control group.
Figures
References
-
- Fong D. T., Hong Y., Chan L. K., Yung P. S., Chan K. M. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007;37(1):73–94. - PubMed
-
- van Rijn R. M., van Os A. G., Bernsen R. M., Luijsterburg P. A., Koes B. W., Bierma-Zeinstra S. M. What is the clinical course of acute ankle sprains? A systematic literature review. Am J Med. 2008;121(4) - PubMed
-
- Hubbard T. J., Kramer L. C., Denegar C. R., Hertel J. Contributing factors to chronic ankle instability. Foot Ankle Int. 2007;28(3):343–354. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
