

Discriminating between latent and active tuberculosis with multiple biomarker responses
- PMID: 21393062
- PMCID: PMC3090479
- DOI: 10.1016/j.tube.2011.02.006
Discriminating between latent and active tuberculosis with multiple biomarker responses
Abstract
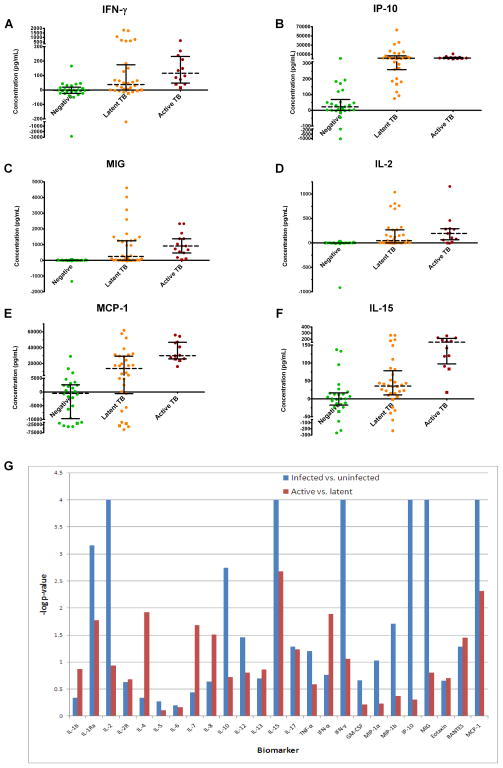
We sought to identify biomarker responses to tuberculosis specific antigens which could 1) improve the diagnosis of tuberculosis infection and 2) allow the differentiation of active and latent infections. Seventy subjects with active tuberculosis (N = 12), latent tuberculosis (N = 32), or no evidence of tuberculosis infection (N = 26) were evaluated. We used the Luminex Multiplexed Bead Array platform to simultaneously evaluate 25 biomarkers in the supernatant of whole blood samples following overnight stimulation using the Quantiferon(®) Gold In-Tube kit. We defined the response to stimulation as the difference (within an individual patient) between the response to the pooled tuberculosis antigens and the negative control. IP-10 response was significantly higher in tuberculosis-infected (active or latent) subjects compared to the uninfected group (p < 0.0001). Among the 25 parameters, expression levels of IL-15 and MCP-1 were found to be significantly higher in the active tuberculosis group compared to the latent tuberculosis group (p = 0.0006 and 0.0030, respectively). When combined, IL-15 and MCP-1 accurately identified 83% of active and 88% of latent infections. The combination of IL-15 and MCP-1 responses was accurate in distinguishing persons with active tuberculosis from persons with latent tuberculosis in this study.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
 ) than non-infected controls (
) than non-infected controls ( ) but do not significantly differ when active TB subjects are compared to latent TB subjects (
) but do not significantly differ when active TB subjects are compared to latent TB subjects ( ) following TB antigen stimulation of whole blood. MCP-1 (E) and IL-15 (F) secretion are significantly increased following TB antigen stimulation of whole blood in TB infected subjects compared with non-infected controls. These biomarkers are also more highly secreted in active TB subjects than latent TB subjects. Each data point represents the concentration observed following stimulation minus the concentration observed in the negative control condition. HIV positive subjects are denoted by squares. Log p-values from Wilcoxon-rank sum tests comparing biomarker secretion in TB infected subjects to non-infected controls (blue bars) as well as active TB subjects to latent TB subjects (red bars) are also plotted (G). The line (log P=3) represents the Bonferroni-corrected significance threshold (50 comparisons).
) following TB antigen stimulation of whole blood. MCP-1 (E) and IL-15 (F) secretion are significantly increased following TB antigen stimulation of whole blood in TB infected subjects compared with non-infected controls. These biomarkers are also more highly secreted in active TB subjects than latent TB subjects. Each data point represents the concentration observed following stimulation minus the concentration observed in the negative control condition. HIV positive subjects are denoted by squares. Log p-values from Wilcoxon-rank sum tests comparing biomarker secretion in TB infected subjects to non-infected controls (blue bars) as well as active TB subjects to latent TB subjects (red bars) are also plotted (G). The line (log P=3) represents the Bonferroni-corrected significance threshold (50 comparisons).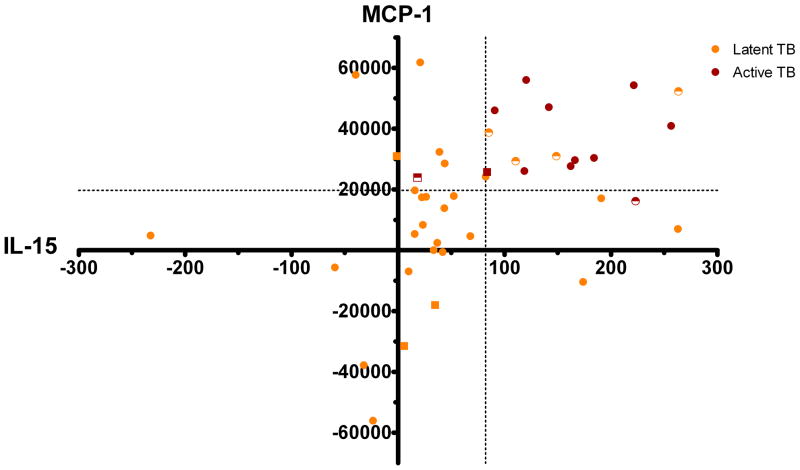 ) and 28/32 (88%) latent TB subjects () were correctly identified. Incorrectly identified subjects are shown as half-shaded shapes. HIV positive subjects are denoted by squares.
) and 28/32 (88%) latent TB subjects () were correctly identified. Incorrectly identified subjects are shown as half-shaded shapes. HIV positive subjects are denoted by squares.References
-
- Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC. Consensus statement. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA. 1999;282(7):677–86. - PubMed
-
- World Health O. Global tuberculosis control 2009 - epidemiology, strategy, financing. 2009 Available from: www.who.int/tb/publications/global_report/2009/pdf/full_report.pdf.
-
- Harries AD, Dye C. Tuberculosis. Annals of Tropical Medicine & Parasitology. 2006;100(5/6):415–31. - PubMed
-
- Sutherland I, Svandová E, Radhakrishna S. The development of clinical tuberculosis following infection with tubercle bacilli: 1. A theoretical model for the development of clinical tuberculosis following infection, linking from data on the risk of tuberculous infection and the incidence of clinical tuberculosis in the Netherlands. Tubercle. 1982;63(4):255–68. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
