

Endovascular treatment of wide-neck intracranial aneurysms using a microcatheter protective technique: results and outcomes in 75 aneurysms
- PMID: 21393400
- PMCID: PMC7965538
- DOI: 10.3174/ajnr.A2411
Endovascular treatment of wide-neck intracranial aneurysms using a microcatheter protective technique: results and outcomes in 75 aneurysms
Abstract
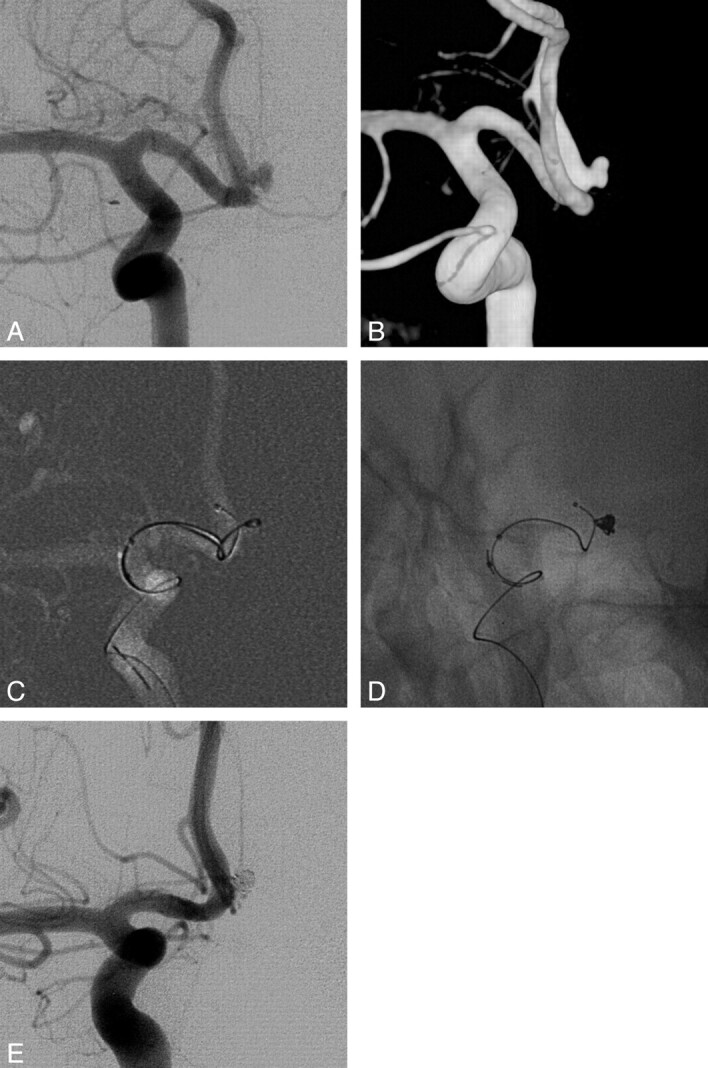
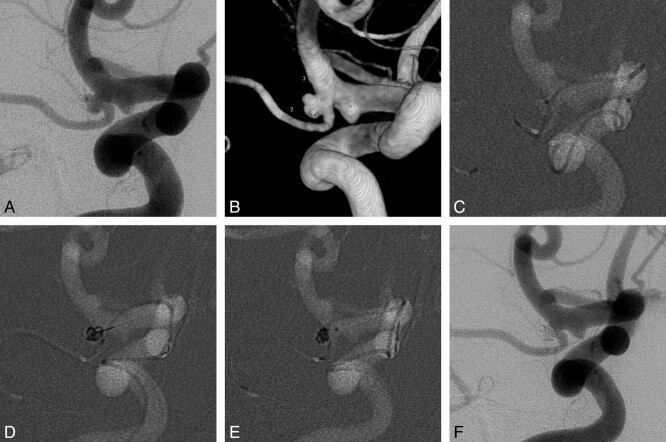
Background and purpose: The microcatheter protective technique positions an additional microcatheter in the parent or side-branching artery to protect it during coil embolization. The purpose of this study was to describe this method and to evaluate its efficacy and safety as an alternative to a multiple-microcatheter or balloon- or stent-assisted technique for wide-neck aneurysms.
Materials and methods: A retrospective review of 74 patients (43 women; mean age, 59.6 years) with 75 wide-neck aneurysms treated with the microcatheter protective technique between January 2003 and April 2010 was performed. Immediate postembolization angiograms were evaluated by using a conventional angiographic scale, and clinical evaluation was performed by using the GOS. Clinical and imaging follow-up were available in 57 (76%) patients, with a mean of 14.7 months.
Results: Postembolization angiograms demonstrated total occlusion in 45 of 75 (60%) aneurysms, a neck remnant in 17 (22.7%), and body filling in 13 (17.3%). The technique-related complication rate was 17.4% (13/75), and the procedural-related morbidity rate was 1.3% (1/74). All patients, except 3 complicated cases with a GOS of <4, had a GOS of 5 at the end of the study period. Of the 57 aneurysms with follow-up, recanalization developed in 5 (8.8%) aneurysms, and 3 (5.3%) cases of major recanalization were re-treated endovascularly.
Conclusions: The microcatheter protective technique is feasible and safe for coil embolization of wide-neck aneurysms, especially in cases that are not suitable for multiple catheter or balloon- or stent-assisted techniques.
Figures

References
-
- Biondi A, Janardhan V, Katz JM, et al. . Neuroform stent-assisted coil embolization of wide-neck intracranial aneurysms: strategies in stent deployment and midterm follow-up. Neurosurgery 2007; 61: 460–68, discussion 468–69 - PubMed
-
- Sluzewski M, van Rooij WJ, Beute GN, et al. . Balloon-assisted coil embolization of intracranial aneurysms: incidence, complications, and angiography results. J Neurosurg 2006; 105: 396–99 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous