

Survival in pediatric dialysis and transplant patients
- PMID: 21393491
- PMCID: PMC3087776
- DOI: 10.2215/CJN.04920610
Survival in pediatric dialysis and transplant patients
Abstract
Background and objectives: Long-term follow-up data are few in children with ESRD. We sought to describe long-term survival, assess risk factors for death, and compare survival between two time periods in pediatric ESRD patients.
Design, setting, participants, & measurements: We used a population-based retrospective cohort utilizing data from a national organ failure registry and from Canada's universal healthcare system. We included 843 children (ages, 0 to 18) initiating renal replacement therapy from 1992 to 2007 and followed them until death or date of last contact (median follow-up, 6.8 years; interquartile range, 3.0 to 10.6). We assessed risk factors for death and examined cause-specific mortality.
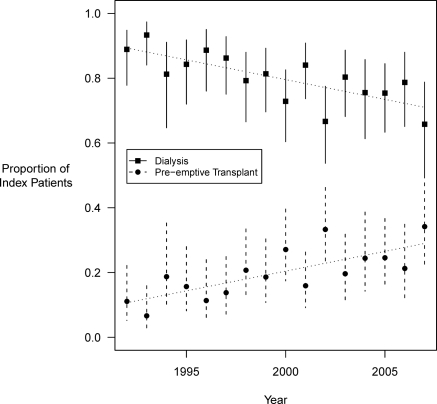
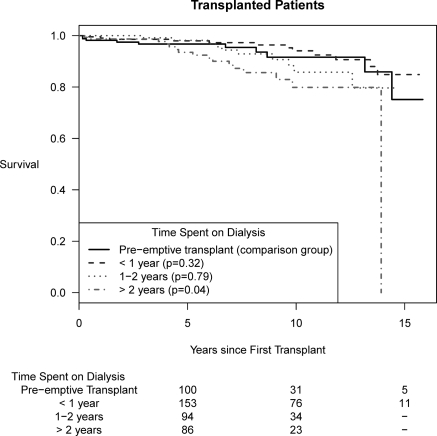
Results: During 5991 patient-years of follow-up, 107 (12.7%) patients died. Unadjusted cumulative survival for the cohort was: 91.7% (95% CI, 89.8 to 93.7%) at 5 years and 85.8% (95% CI, 82.8 to 88.8%) at 10 years. Among patients commencing dialysis, overall adjusted survival was poorest among those who started dialysis at age <1 year. No secular trends in survival were noted for either dialysis or transplant patients. The proportion of incident patients receiving pre-emptive transplantation increased over time. Pre-emptively transplanted patients did not demonstrate superior adjusted survival compared with those who spent >2 years on dialysis before transplant (hazard ratio, 1.53; 95% CI, 0.63 to 3.67).
Conclusions: No significant improvements in survival were observed among ESRD patients over the study period. Time with transplant function had the strongest association with survival. Pre-emptive transplantation was not associated with improved survival in adjusted models.
Copyright © 2011 by the American Society of Nephrology
Figures
References
-
- McDonald SP, Craig JC: Long-term survival of children with end-stage renal disease. N Engl J Med 350: 2654–2662, 2004 - PubMed
-
- Johnstone LM, Jones CL, Grigg LE, Wilkinson JL, Walker RG, Powell HR: Left ventricular abnormalities in children, adolescents and young adults with renal disease. Kidney Int 50: 998–1006, 1996 - PubMed
-
- Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y, Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB: Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med 342: 1478–1483, 2000 - PubMed
-
- Bartosh SM, Leverson G, Robillard D, Sollinger HW: Long-term outcomes in pediatric renal transplant recipients who survive into adulthood. Transplantation 76: 1195–1200, 2003 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
