

Continuous femoral nerve blocks: varying local anesthetic delivery method (bolus versus basal) to minimize quadriceps motor block while maintaining sensory block
- PMID: 21394001
- PMCID: PMC3116995
- DOI: 10.1097/ALN.0b013e3182124dc6
Continuous femoral nerve blocks: varying local anesthetic delivery method (bolus versus basal) to minimize quadriceps motor block while maintaining sensory block
Abstract
Background: Whether the method of local anesthetic administration for continuous femoral nerve blocks--basal infusion versus repeated hourly bolus doses--influences block effects remains unknown.
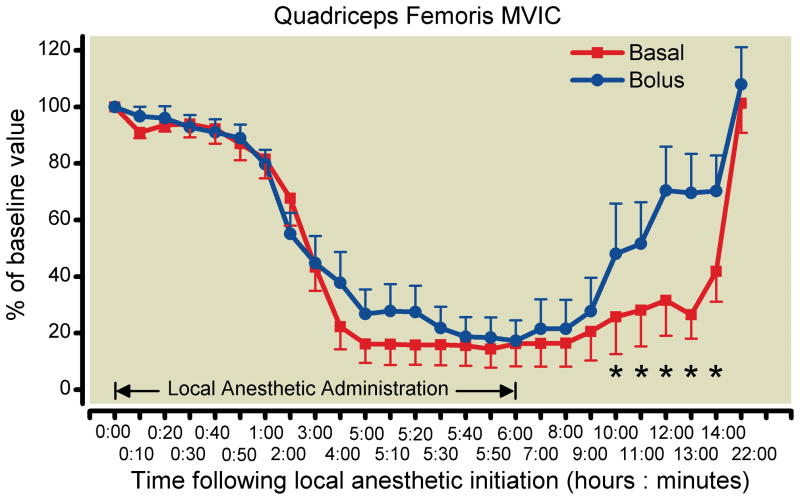
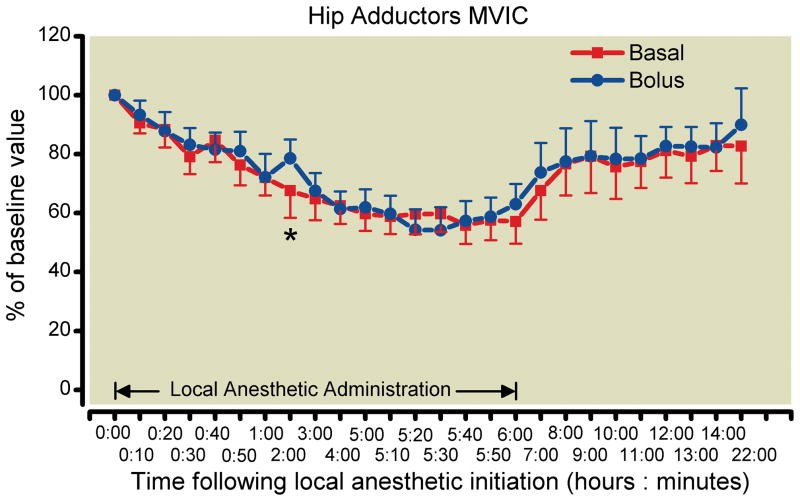
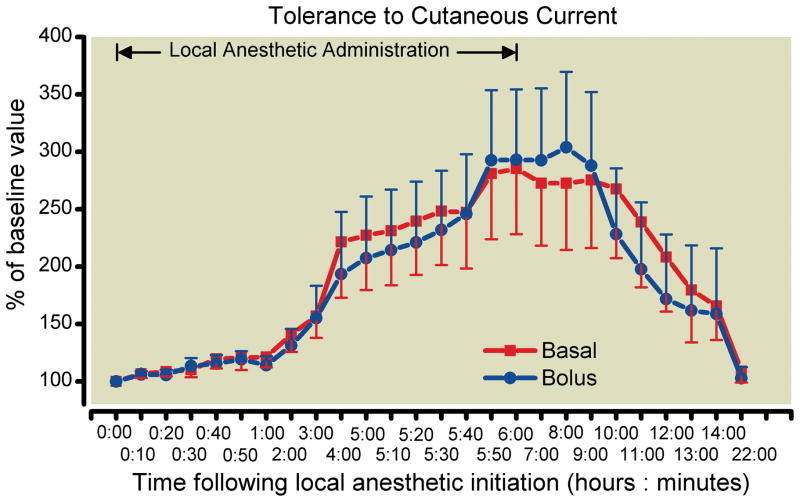
Methods: Bilateral femoral perineural catheters were inserted in volunteers (n = 11). Ropivacaine 0.1% was concurrently administered through both catheters: a 6-h continuous 5 ml/h basal infusion on one side and 6 hourly bolus doses on the contralateral side. The primary endpoint was the maximum voluntary isometric contraction (MVIC) of the quadriceps femoris muscle at hour 6. Secondary endpoints included quadriceps MVIC at other time points, hip adductor MVIC, and cutaneous sensation 2 cm medial to the distal quadriceps tendon in the 22 h after initiation of local anesthetic administration.
Results: Quadriceps MVIC for limbs receiving 0.1% ropivacaine as a basal infusion declined by a mean (SD) of 84% (19) compared with 83% (24) for those receiving 0.1% ropivacaine as repeated bolus doses between baseline and hour 6 (paired t test P = 0.91). Intrasubject comparisons (left vs. right) also reflected a lack of difference: the mean basal-bolus difference in quadriceps MVIC at hour 6 was -1.1% (95% CI -22.0-19.8%). The similarity did not reach the a priori threshold for concluding equivalence, which was the 95% CI decreasing within ± 20%. There were similar minimal differences in the secondary endpoints during local anesthetic administration.
Conclusions: This study did not find evidence to support the hypothesis that varying the method of local anesthetic administration--basal infusion versus repeated bolus doses--influences continuous femoral nerve block effects to a clinically significant degree.
Conflict of interest statement
Conflict of Interest: None.
Figures

Comment in
-
Multiorifice catheters are required to maximize the benefits of intermittent bolus continuous regional techniques.Anesthesiology. 2012 May;116(5):1154; author reply 1154-6. doi: 10.1097/ALN.0b013e31824de982. Anesthesiology. 2012. PMID: 22531255 No abstract available.
References
-
- Ilfeld BM, Mariano ER, Girard PJ, Loland VJ, Meyer RS, Donovan JF, Pugh GA, Le LT, Sessler DI, Shuster JJ, Theriaque DW, Ball ST. A multicenter, randomized, triple-masked, placebo-controlled trial of the effect of ambulatory continuous femoral nerve blocks on discharge-readiness following total knee arthroplasty in patients on general orthopaedic wards. Pain. 2010;150:477–84. - PMC - PubMed
-
- Ilfeld BM, Yaksh TL. The end of postoperative pain–a fast-approaching possibility? And, if so, will we be ready? Reg Anesth Pain Med. 2009;34:85–7. - PubMed
-
- Borgeat A, Kalberer F, Jacob H, Ruetsch YA, Gerber C. Patient-controlled interscalene analgesia with ropivacaine 0.2% versus bupivacaine 0.15% after major open shoulder surgery: The effects on hand motor function. AnesthAnalg. 2001;92:218–23. - PubMed
-
- Kandasami M, Kinninmonth AW, Sarungi M, Baines J, Scott NB. Femoral nerve block for total knee replacement - A word of caution. Knee. 2009;16:98–100. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
