

Is total ankle arthroplasty a cost-effective alternative to ankle fusion?
- PMID: 21394559
- PMCID: PMC3094612
- DOI: 10.1007/s11999-011-1848-4
Is total ankle arthroplasty a cost-effective alternative to ankle fusion?
Abstract
Background: Total ankle arthroplasty (TAA) implantation is increasing, as the potential for pain relief and restoration of function and risks are compared with those for ankle fusion. A previous analysis with a simple decision tree suggested TAA was cost-effective compared with ankle fusion. However, reevaluation is warranted with the availability of newer, more costly implants and longer-term patient followup data.
Questions/purposes: Considering all direct medical costs regardless of the payer, we determined if TAA remains a cost-effective alternative to ankle fusion when updated evidence is considered.
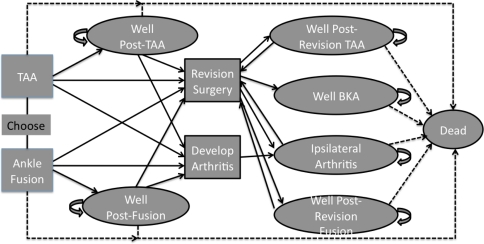
Patients and methods: Using a Markov model, we evaluated expected costs and quality-adjusted life years (QALY) for a 60-year-old hypothetical cohort with end-stage ankle arthritis treated with either TAA or ankle fusion. Costs were estimated from 2007 diagnosis-related group (DRG) and current procedural terminology (CPT) codes for each procedure. Rates were extracted from the literature. The incremental cost-effectiveness ratio (ICER), a measure of added cost divided by QALY gained for TAA relative to ankle fusion, was estimated. To identify factors affecting the value of TAA, sensitivity analyses were performed on all variables.
Results: TAA costs $20,200 more than ankle fusion and resulted in 1.7 additional QALY, with an ICER of $11,800/QALY gained. Few variables in the sensitivity analyses resulted in TAA no longer being cost-effective.
Conclusion: Despite more costly implants and longer followup, TAA remains a cost-effective alternative to ankle fusion in a 60-year-old cohort with end-stage ankle arthritis.
Figures
References
-
- Anderson T, Montgomery F, Carlsson A. Uncemented STAR total ankle prostheses: three to eight-year follow-up of fifty-one consecutive ankles. J Bone Joint Surg Am. 2003;85:1321–1329. - PubMed
-
- Arias E. United States life tables, 2004. Natl Vital Stat Rep. 2007;56:1–39. - PubMed
-
- Coester LM, Saltzman CL, Leupold J, Pontarelli W. Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am. 2001;83:219–228. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
