

Review
doi: 10.2217/imt.10.114.
Cancer radioimmunotherapy
Affiliations
- PMID: 21395378
- PMCID: PMC3123828
- DOI: 10.2217/imt.10.114
Item in Clipboard
Review
Cancer radioimmunotherapy
Immunotherapy.
2011 Mar.
Abstract
Targeting of radionuclides with antibodies, or radioimmunotherapy, has been an active field of research spanning nearly 50 years, evolving with advancing technologies in molecular biology and chemistry, and with many important preclinical and clinical studies illustrating the benefits, but also the challenges, which all forms of targeted therapies face. There are currently two radiolabeled antibodies approved for the treatment of non-Hodgkin lymphoma, but radioimmunotherapy of solid tumors remains a challenge. Novel antibody constructs, focusing on treatment of localized and minimal disease, and pretargeting are all promising new approaches that are currently under investigation.
Figures
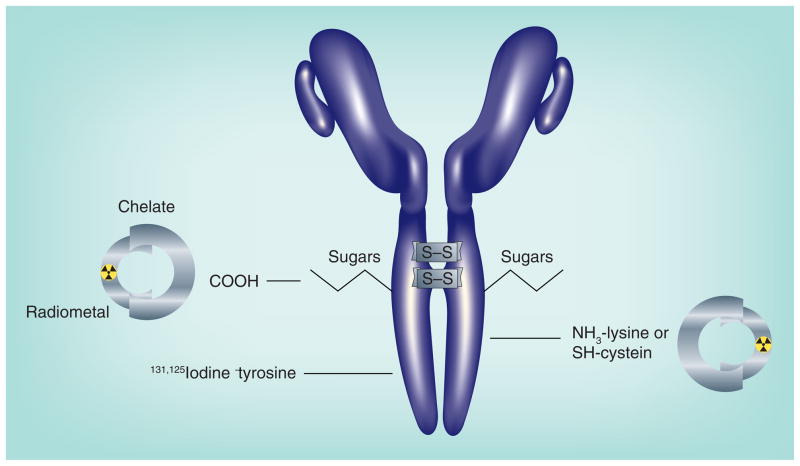
Radioiodine is bound to aromatic rings, primarily to tyrosine, in the presence of a mild oxidative agent, such as iodogen or chloramine-T. The ε amino group of lysine can be modified to accept a metal-binding chelate, which is then loaded with a radiometal. Exposing IgG to a mild reducing agent can split disulfide bonds, allowing the coupling of chelate or other compounds to the reactive sulfhydryl. To ensure amino acids within the antigen-binding sites of the antibody are not altered, carbohydrates, commonly found on the IgG’s CH2 domain, can be modified to accept a chelate.
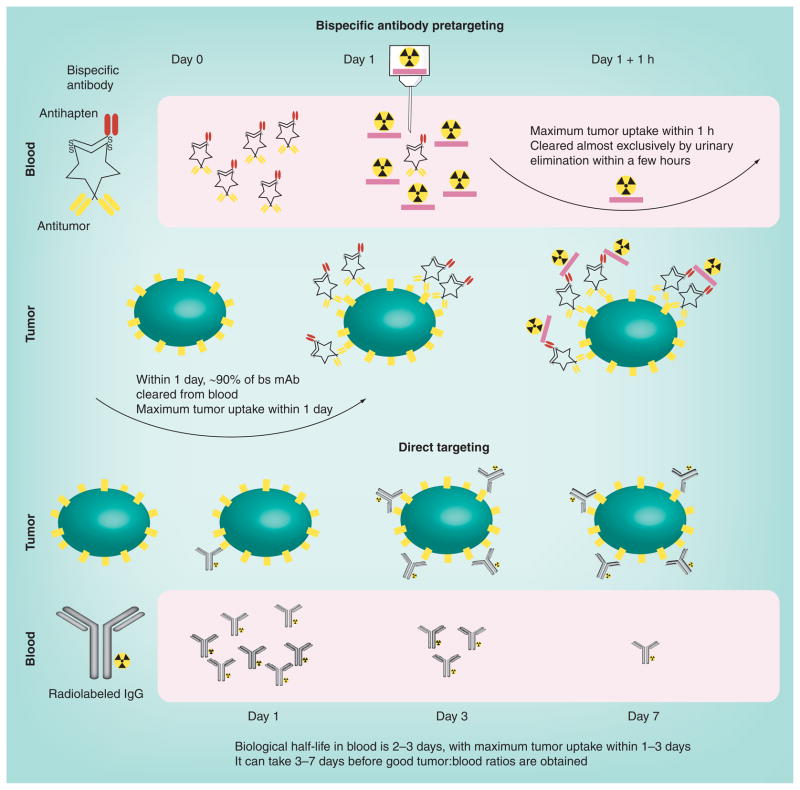
For pretargeting, an unlabeled bs mAb is used (shown is a tri-Fab recombinant structure described in Figure 3). In patients, 90% of this antibody is cleared from the blood, and animal studies have demonstrated that maximum tumor uptake occurs within approximately 6 h. The radioactivity is introduced on a small peptide (~four amino acids) that contains two haptens to help stabilize binding within the tumor (affinity enhancement). The peptide also contains structures that will bind the radionuclide. The radiolabeled hapten–peptide is administered when the bs mAb is sufficiently cleared from the blood, and clears exceptionally fast from the blood and body by urinary excretion, reaching peak tumor uptake within 1 h. Tumor:blood ratios are highly favorable within a few hours. In direct targeting, the isotope is on the antibody. Shown here is an IgG that will clear very slowly from the blood, gradually building its concentration in the tumor, so tumor:blood ratios remain relatively low over the first few days. bs mAb: Bispecific monoclonal antibody.
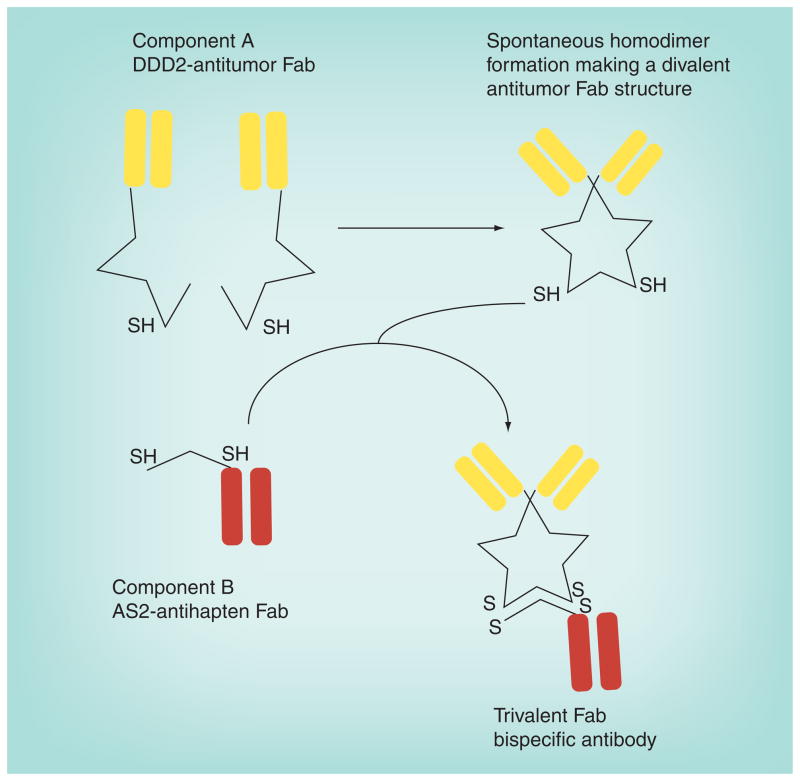
The bs mAb consists of two proteins. The first is a Fab, specific for a tumor antigen, modified with a peptide structure known as the DDD, which was modified to introduce a cysteine residue in a strategic location (DDD2). The DDD2 residues have a natural affinity for binding to each other to form homodimers, resulting in a divalent Fab structure. The second protein is the Fab modified with an anchoring domain (AD) that will specifically dock within the dimerized DDD2 structure. The AD segment also had cysteine residues strategically placed so that when the docking occurs, the cysteine residues on the DDD2 and AD2 will lock into place. bs mAb: Bispecific monoclonal antibody; DDD: Dimerization docking domain. Adapted from [259].
References
-
- Grossbard ML, Press OW, Appelbaum FR, Bernstein ID, Nadler LM. Monoclonal antibody-based therapies of leukemia and lymphoma. Blood. 1992;80(4):863–878. - PubMed
-
- Sharkey RM, Burton J, Goldenberg DM. Radioimmunotherapy of non-Hodgkin’s lymphoma: a critical appraisal. Expert Rev Clin Immunol. 2005;1(1):47–62. - PubMed
-
- Sharkey RM, Goldenberg DM. Perspectives on cancer therapy with radiolabeled monoclonal antibodies. J Nucl Med. 2005;46(Suppl 1):S115–S127. - PubMed
-
- Nelson AL, Dhimolea E, Reichert JM. Development trends for human monoclonal antibody therapeutics. Nat Rev Drug Discov. 2010;9(10):767–774. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources