

Mindfulness-based stress reduction versus pharmacotherapy for chronic primary insomnia: a randomized controlled clinical trial
- PMID: 21397868
- PMCID: PMC3077056
- DOI: 10.1016/j.explore.2010.12.003
Mindfulness-based stress reduction versus pharmacotherapy for chronic primary insomnia: a randomized controlled clinical trial
Abstract
Objective: The aim of this study was to investigate the potential of mindfulness-based stress reduction (MBSR) as a treatment for chronic primary insomnia.
Design: A randomized controlled trial was conducted.
Setting: The study was conducted at a university health center.
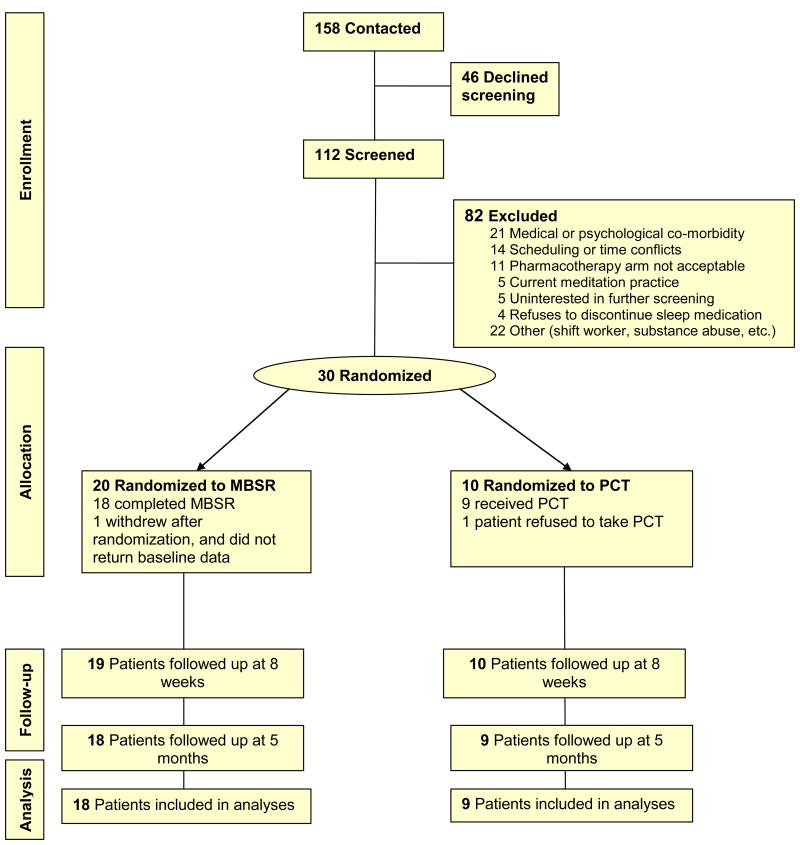
Patients: Thirty adults with primary chronic insomnia based on criteria of the Diagnostic and Statistical Manual of Mental Disorders, Text Revision, 4th Edition were randomized 2:1 to MBSR or pharmacotherapy (PCT).
Interventions: Mindfulness-based stress reduction, a program of mindfulness meditation training consisting of eight weekly 2.5 hour classes and a daylong retreat, was provided, with ongoing home meditation practice expectations during three-month follow-up; PCT, consisting of three milligrams of eszopiclone (LUNESTA) nightly for eight weeks, followed by three months of use as needed. A 10-minute sleep hygiene presentation was included in both interventions.
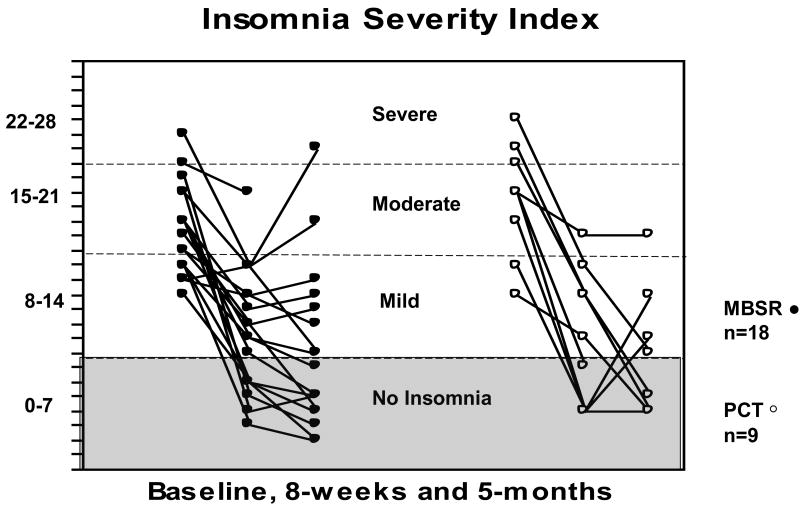
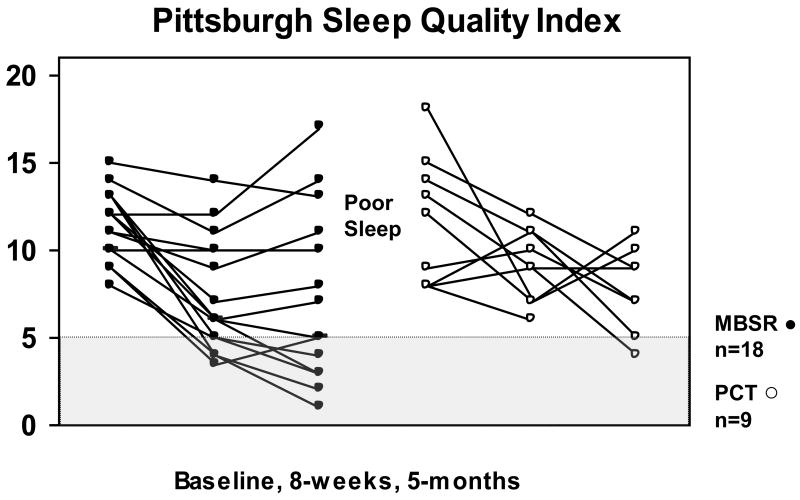
Main outcomes: The Insomnia Severity Index (ISI), Pittsburgh Sleep Quality Index (PSQI), sleep diaries, and wrist actigraphy were collected pretreatment, posttreatment (eight weeks), and at five months (self-reports only).
Results: Between baseline and eight weeks, sleep onset latency (SOL) measured by actigraphy decreased 8.9 minutes in the MBSR arm (P < .05). Large, significant improvements were found on the ISI, PSQI, and diary-measured total sleep time, SOL, and sleep efficiency (P < .01, all) from baseline to five-month follow-up in the MBSR arm. Changes of comparable magnitude were found in the PCT arm. Twenty-seven of 30 patients completed their assigned treatment. This study provides initial evidence for the efficacy of MBSR as a viable treatment for chronic insomnia as measured by sleep diary, actigraphy, well-validated sleep scales, and measures of remission and clinical recovery.
Trial registration: ClinicalTrials.gov NCT00515177.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Buscemi N, Vandermeer B, Friesen C, et al. Summary, Evidence Report/Technology Assessment No. 125. (Prepared by the University of Alberta Evidence-based Practice Center, under Contract No C400000021.) AHRQ Publication No 05-E-021-1. Rockville, MD: Agency for Healthcare Research and Quality; Jun, 2005. Manifestations and management of chronic insomnia in adults. - PMC - PubMed
-
- Ohayon MM. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Medicine Reviews. 2002;6:97–111. - PubMed
-
- . National Institutes of Health State-of-the-Science Conference Final Statement on Manifestations and Management of Chronic Insomnia in Adults. Sleep. 2005;28:1049–57. - PubMed
-
- Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA. 1989;262:1479–84. - PubMed
-
- Mallon L, Broman JE, Hetta J. Sleep complaints predict coronary artery disease mortality in males: a 12-year follow-up study of a middle-aged Swedish population. J Intern Med. 2002;251:207–16. - PubMed
