

Combination of external beam radiotherapy (EBRT) with intratumoral injection of dendritic cells as neo-adjuvant treatment of high-risk soft tissue sarcoma patients
- PMID: 21398051
- PMCID: PMC4241354
- DOI: 10.1016/j.ijrobp.2010.12.068
Combination of external beam radiotherapy (EBRT) with intratumoral injection of dendritic cells as neo-adjuvant treatment of high-risk soft tissue sarcoma patients
Abstract
Purpose: The goal of this study was to determine the effect of combination of intratumoral administration of dendritic cells (DC) and fractionated external beam radiation (EBRT) on tumor-specific immune responses in patients with soft-tissue sarcoma (STS).
Methods and material: Seventeen patients with large (>5 cm) high-grade STS were enrolled in the study. They were treated in the neoadjuvant setting with 5,040 cGy of EBRT, split into 28 fractions and delivered 5 days per week, combined with intratumoral injection of 10(7) DCs followed by complete resection. DCs were injected on the second, third, and fourth Friday of the treatment cycle. Clinical evaluation and immunological assessments were performed.
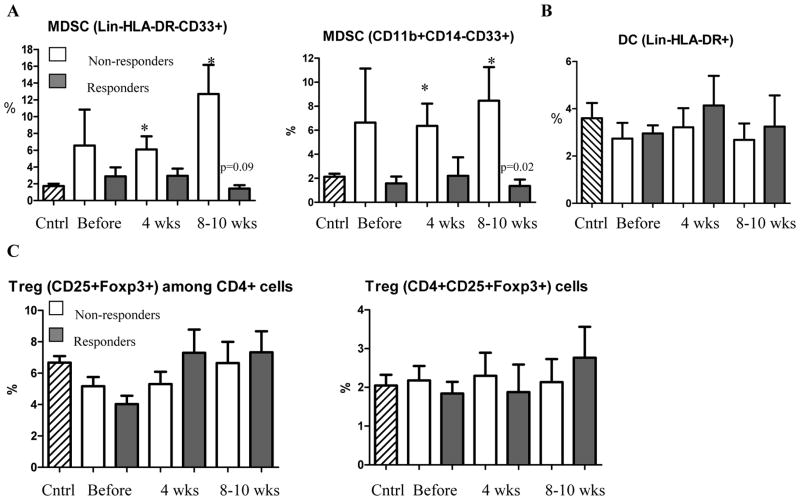
Results: The treatment was well tolerated. No patient had tumor-specific immune responses before combined EBRT/DC therapy; 9 patients (52.9%) developed tumor-specific immune responses, which lasted from 11 to 42 weeks. Twelve of 17 patients (70.6%) were progression free after 1 year. Treatment caused a dramatic accumulation of T cells in the tumor. The presence of CD4(+) T cells in the tumor positively correlated with tumor-specific immune responses that developed following combined therapy. Accumulation of myeloid-derived suppressor cells but not regulatory T cells negatively correlated with the development of tumor-specific immune responses. Experiments with (111)In labeled DCs demonstrated that these antigen presenting cells need at least 48 h to start migrating from tumor site.
Conclusions: Combination of intratumoral DC administration with EBRT was safe and resulted in induction of antitumor immune responses. This suggests that this therapy is promising and needs further testing in clinical trials design to assess clinical efficacy.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
No Actual or potential conflicts of interest exist
Figures



References
-
- Friedman EJ. Immune modulation by ionizing radiation and its implications for cancer immunotherapy. Curr Pharm Des. 2002;8:1765–1780. - PubMed
-
- Quarmby S, Kumar P, Kumar S. Radiation-induced normal tissue injury: role of adhesion molecules in leukocyte-endothelial cell interactions. Int J Cancer. 1999;82:385–395. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
