

A clinical diagnostic model for predicting influenza among young adult military personnel with febrile respiratory illness in Singapore
- PMID: 21399686
- PMCID: PMC3047544
- DOI: 10.1371/journal.pone.0017468
A clinical diagnostic model for predicting influenza among young adult military personnel with febrile respiratory illness in Singapore
Abstract
Introduction: Influenza infections present with wide-ranging clinical features. We aim to compare the differences in presentation between influenza and non-influenza cases among those with febrile respiratory illness (FRI) to determine predictors of influenza infection.
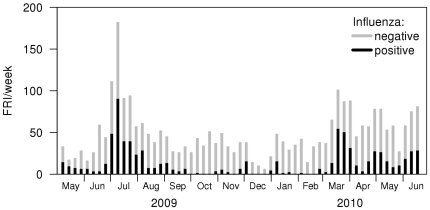
Methods: Personnel with FRI (defined as fever ≥ 37.5 °C, with cough or sore throat) were recruited from the sentinel surveillance system in the Singapore military. Nasal washes were collected, and tested using the Resplex II and additional PCR assays for etiological determination. Interviewer-administered questionnaires collected information on patient demographics and clinical features. Univariate comparison of the various parameters was conducted, with statistically significant parameters entered into a multivariate logistic regression model. The final multivariate model for influenza versus non-influenza cases was used to build a predictive probability clinical diagnostic model.
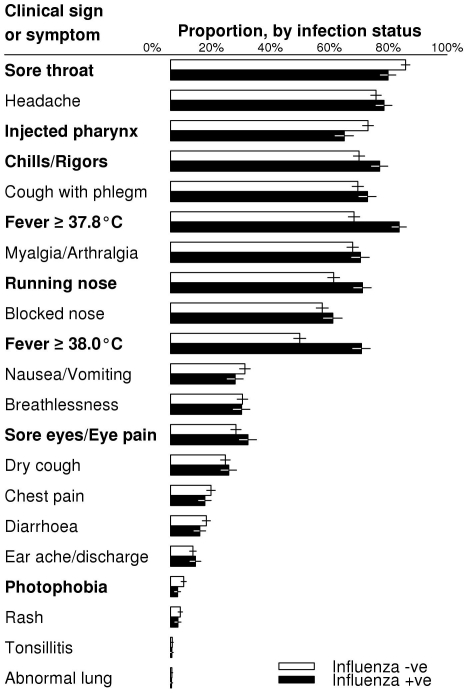
Results: 821 out of 2858 subjects recruited from 11 May 2009 to 25 Jun 2010 had influenza, of which 434 (52.9%) had 2009 influenza A (H1N1), 58 (7.1%) seasonal influenza A (H3N2) and 269 (32.8%) influenza B. Influenza-positive cases were significantly more likely to present with running nose, chills and rigors, ocular symptoms and higher temperature, and less likely with sore throat, photophobia, injected pharynx, and nausea/vomiting. Our clinical diagnostic model had a sensitivity of 65% (95% CI: 58%, 72%), specificity of 69% (95% CI: 62%, 75%), and overall accuracy of 68% (95% CI: 64%, 71%), performing significantly better than conventional influenza-like illness (ILI) criteria.
Conclusions: Use of a clinical diagnostic model may help predict influenza better than the conventional ILI definition among young adults with FRI.
Conflict of interest statement
Figures
References
-
- Chen MI, Lee VJ, Lim WY, Barr IG, Lin RT, et al. 2009 influenza A(H1N1) seroconversion rates and risk factors among distinct adult cohorts in Singapore. JAMA. 2010;303(14):1383–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
