

Inability of providers to predict unplanned readmissions
- PMID: 21399994
- PMCID: PMC3138589
- DOI: 10.1007/s11606-011-1663-3
Inability of providers to predict unplanned readmissions
Abstract
Background: Readmissions cause significant distress to patients and considerable financial costs. Identifying hospitalized patients at high risk for readmission is an important strategy in reducing readmissions. We aimed to evaluate how well physicians, case managers, and nurses can predict whether their older patients will be readmitted and to compare their predictions to a standardized risk tool (Probability of Repeat Admission, or P(ra)).
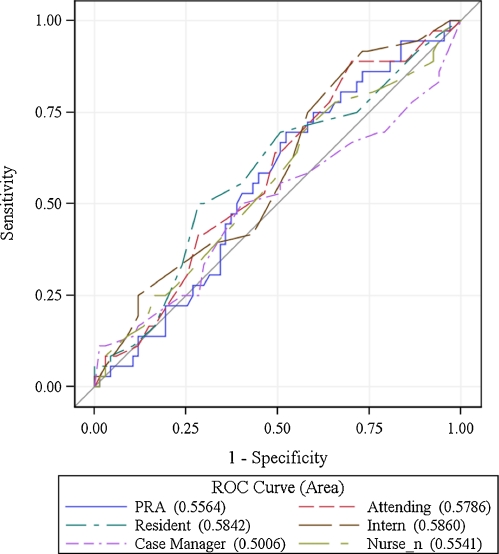
Methods: Patients aged ≥ 65 discharged from the general medical service at University of California, San Francisco Medical Center, a 550-bed tertiary care academic medical center, were eligible for enrollment over a 5-week period. At the time of discharge, the inpatient team members caring for each patient estimated the chance of unscheduled readmission within 30 days and predicted the reason for potential readmission. We also calculated the P(ra) for each patient. We identified readmissions through electronic medical record (EMR) review and phone calls with patients/caregivers. Discrimination was determined by creating ROC curves for each provider group and the P(ra).
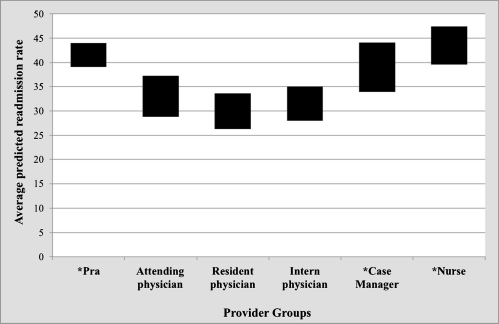
Results: One hundred sixty-four patients were eligible for enrollment. Of these patients, five died during the 30-day period post-discharge. Of the remaining 159 patients, 52 patients (32.7%) were readmitted. Mean readmission predictions for the physician providers were closest to the actual readmission rate, while case managers, nurses, and the P(ra) all overestimated readmissions. The ability to discriminate between readmissions and non-readmissions was poor for all provider groups and the P(ra) (AUC from 0.50 for case managers to 0.59 for interns, 0.56 for P(ra)). None of the provider groups predicted the reason for readmission with accuracy.
Conclusions: This study found (1) overall readmission rates were higher than previously reported, possibly because we employed a more thorough follow-up methodology, and (2) neither providers nor a published algorithm were able to accurately predict which patients were at highest risk of readmission. Amid increasing pressure to reduce readmission rates, hospitals do not have accurate predictive tools to guide their efforts.
Figures
References
-
- A New Era of Responsibility: Renewing America’s Promise. http://www.whitehouse.gov/omb/assets/fy2010_new_era/A_New_Era_of_Respons... Accessed February 2, 2011.
-
- U.S. Department of Health & Human Services. http://www.hospitalcompare.hhs.gov. Accessed February 2, 2011.
-
- University HealthSystem Consortium. https://www.uhc.edu/. Accessed February 2, 2011.
-
- A path to bundled payment around a rehospitalization.: Medicare payment Advisory Commission; June 2005.
-
- Copeland-Fields L, Griffin T, Jenkins T, Buckley M, Wise LC. Comparison of outcome predictions made by physicians, by nurses, and by using the Mortality Prediction Model. Am J Crit Care. 2001;10(5):313–319. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
