

Assessment of disease-severity scoring systems for patients with sepsis in general internal medicine departments
- PMID: 21401927
- PMCID: PMC3219360
- DOI: 10.1186/cc10102
Assessment of disease-severity scoring systems for patients with sepsis in general internal medicine departments
Abstract
Introduction: Due to the increasing burden on hospital systems, most elderly patients with non-surgical sepsis are admitted to general internal medicine departments. Disease-severity scoring systems are used for stratification of patients for utilization management, performance assessment, and clinical research. Some widely used scoring systems for septic patients are inappropriate when rating non-surgical patients in a non-intensive care unit (ICU) environment mainly because their calculations require types of data that are frequently unavailable. This study aimed to assess the fitness of four scoring systems for septic patients hospitalized in general internal medicine departments: modified early warning score (MEWS), simple clinical score (SCS), mortality in emergency department sepsis (MEDS) score, and rapid emergency medicine score (REMS).
Methods: We prospectively collected computerized data of septic patients admitted to general internal medicine departments in our community-based university hospital. We followed 28-day in-hospital mortality, overall in-hospital mortality, and 30- and 60-day mortality. Using a logistic regression procedure we calculated the area under ROC curve (AUC) for every scoring system.
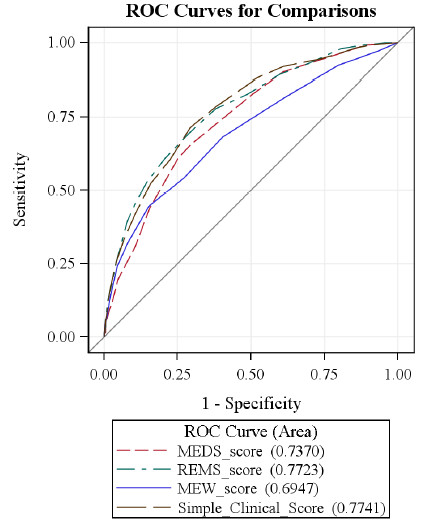
Results: Between February 1st, 2008 and April 30th, 2009 we gathered data of 1,072 patients meeting sepsis criteria on admission to general internal medicine departments. The 28-day mortality was 19.4%. The AUC for the MEWS was 0.65-0.70, for the SCS 0.76-0.79, for the MEDS 0.73-0.75, and for the REMS, 0.74-0.79. Using Hosmer-Lemeshow statistics, a lack of fit was found for the MEDS model. All scoring systems performed better than calculations based on sepsis severity.
Conclusions: The SCS and REMS are the most appropriate clinical scores to predict the mortality of patients with sepsis in general internal medicine departments.
Figures
References
-
- Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: final data for 2006. Natl Vital Stat Rep. 2009;57:1–136. - PubMed
-
- Esteban A, Frutos-Vivar F, Ferguson ND, Peñuelas O, Lorente JA, Gordo F, Honrubia T, Algora A, Bustos A, García G, Diaz-Regañón IR, de Luna RR. Sepsis incidence and outcome: contrasting the intensive care unit with the hospital ward. Crit Care Med. 2007;35:1284–1289. doi: 10.1097/01.CCM.0000260960.94300.DE. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
