

Postoperative cognitive deficit after cardiopulmonary bypass with preserved cerebral oxygenation: a prospective observational pilot study
- PMID: 21401948
- PMCID: PMC3068111
- DOI: 10.1186/1471-2253-11-7
Postoperative cognitive deficit after cardiopulmonary bypass with preserved cerebral oxygenation: a prospective observational pilot study
Abstract
Background: Neurologic deficits after cardiac surgery are common complications. Aim of this prospective observational pilot study was to investigate the incidence of postoperative cognitive deficit (POCD) after cardiac surgery, provided that relevant decrease of cerebral oxygen saturation (cSO2) is avoided during cardiopulmonary bypass.
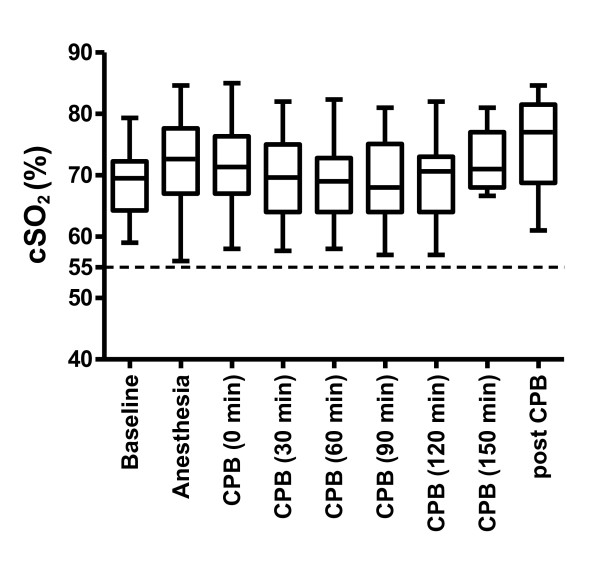
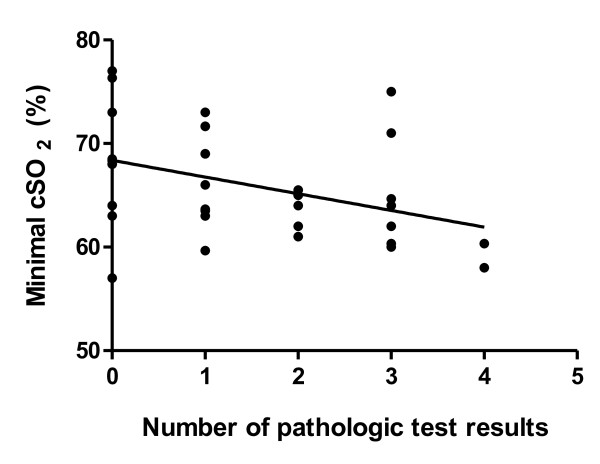
Methods: cSO2 was measured by near infrared spectroscopy in 35 patients during cardiopulmonary bypass. cSO2 was kept above 80% of baseline and above 55% during anesthesia including cardiopulmonary bypass. POCD was tested by trail making test, digit symbol substitution test, Ray's auditorial verbal learning test, digit span test and verbal fluency test the day before and 5 days after surgery. POCD was defined as a decline in test performance that exceeded - 20% from baseline in two tests or more. Correlation of POCD with lowest cSO2 and cSO2 - threshold were determined explorative.
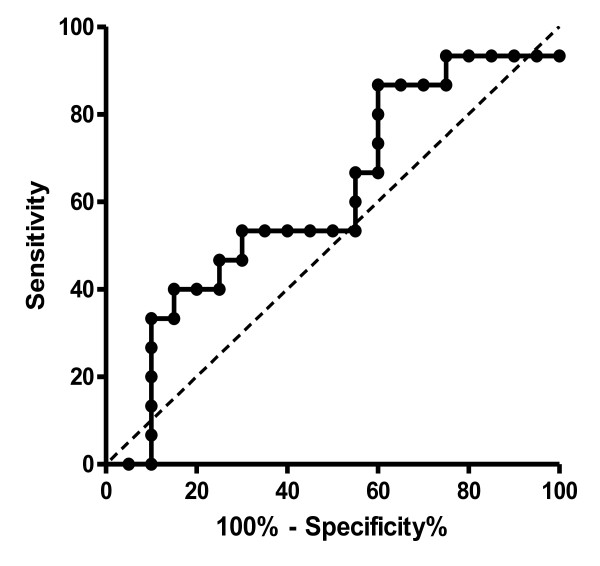
Results: POCD was observed in 43% of patients. Lowest cSO2 during cardiopulmonary bypass was significantly correlated with POCD (p = 0.015, r2 = 0.44, without Bonferroni correction). A threshold of 65% for cSO2 was able to predict POCD with a sensitivity of 86.7% and a specificity of 65.0% (p = 0.03, without Bonferroni correction).
Conclusions: Despite a relevant decrease of cerebral oxygen saturation was avoided in our pilot study during cardiopulmonary bypass, incidence of POCD was comparable to that reported in patients without monitoring. A higher threshold for cSO2 may be needed to reduce the incidence of POCD.
Figures
References
-
- Roach GW, Kanchuger M, Mangano CM, Newman M, Nussmeier N, Wolman R, Aggarwal A, Marschall K, Graham SH, Ley C. Adverse cerebral outcomes after coronary bypass surgery. Multicenter Study of Perioperative Ischemia Research Group and the Ischemia Research and Education Foundation Investigators. The New England journal of medicine. 1996;335(25):1857–1863. doi: 10.1056/NEJM199612193352501. - DOI - PubMed
-
- Newman MF, Kirchner JL, Phillips-Bute B, Gaver V, Grocott H, Jones RH, Mark DB, Reves JG, Blumenthal JA. Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. The New England journal of medicine. 2001;344(6):395–402. doi: 10.1056/NEJM200102083440601. - DOI - PubMed
-
- Mackensen GB. Cerebral dysfunction - Pathophysiology of central nervous functions. Appl Cardiopulm Pathophysiol. 2009;13:146–147.
-
- Phillips-Bute B, Mathew JP, Blumenthal JA, Grocott HP, Laskowitz DT, Jones RH, Mark DB, Newman MF. Association of neurocognitive function and quality of life 1 year after coronary artery bypass graft (CABG) surgery. Psychosomatic medicine. 2006;68(3):369–375. doi: 10.1097/01.psy.0000221272.77984.e2. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
