

Time course of the attenuation effect of repeated antipsychotic treatment on prepulse inhibition disruption induced by repeated phencyclidine treatment
- PMID: 21402097
- PMCID: PMC3081992
- DOI: 10.1016/j.pbb.2011.03.007
Time course of the attenuation effect of repeated antipsychotic treatment on prepulse inhibition disruption induced by repeated phencyclidine treatment
Abstract
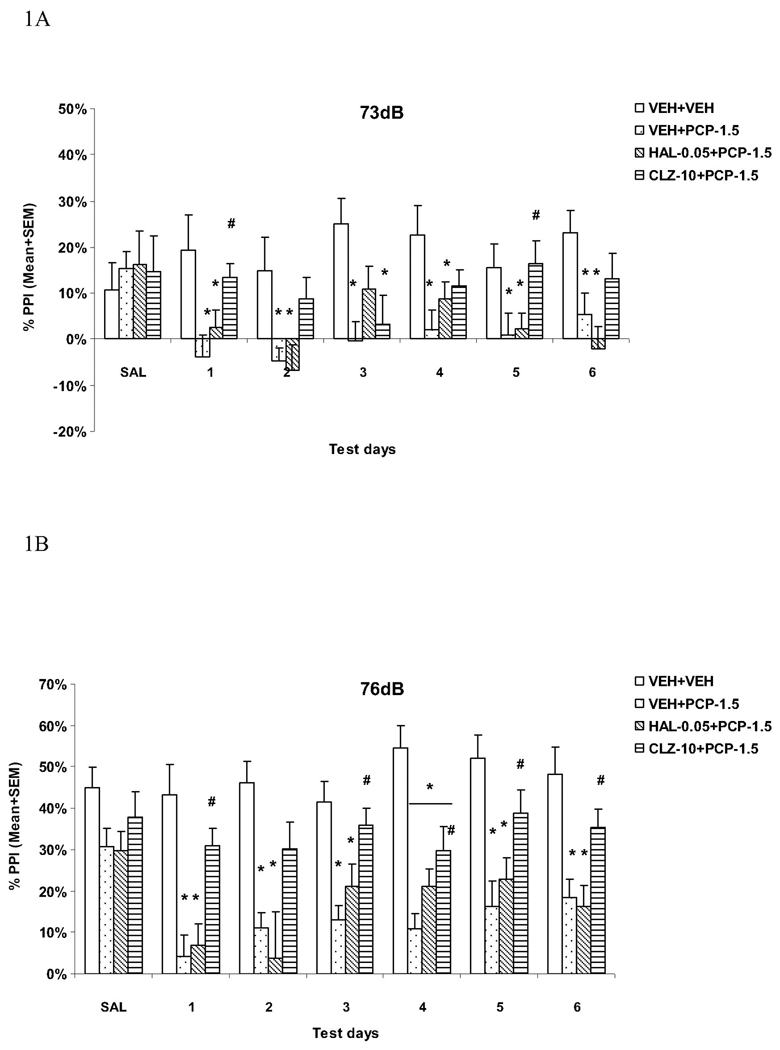
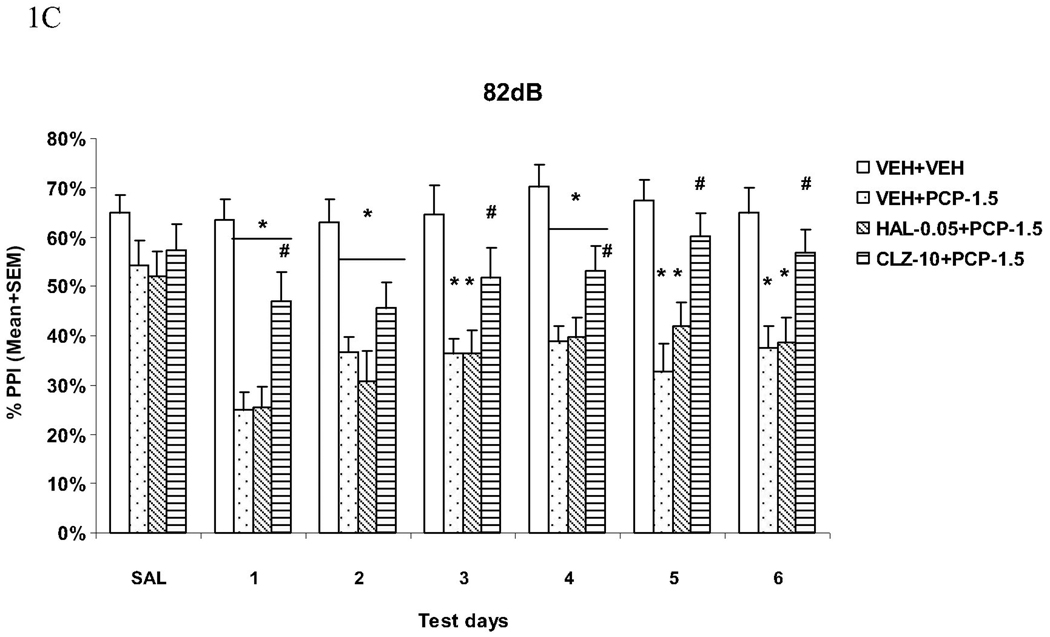
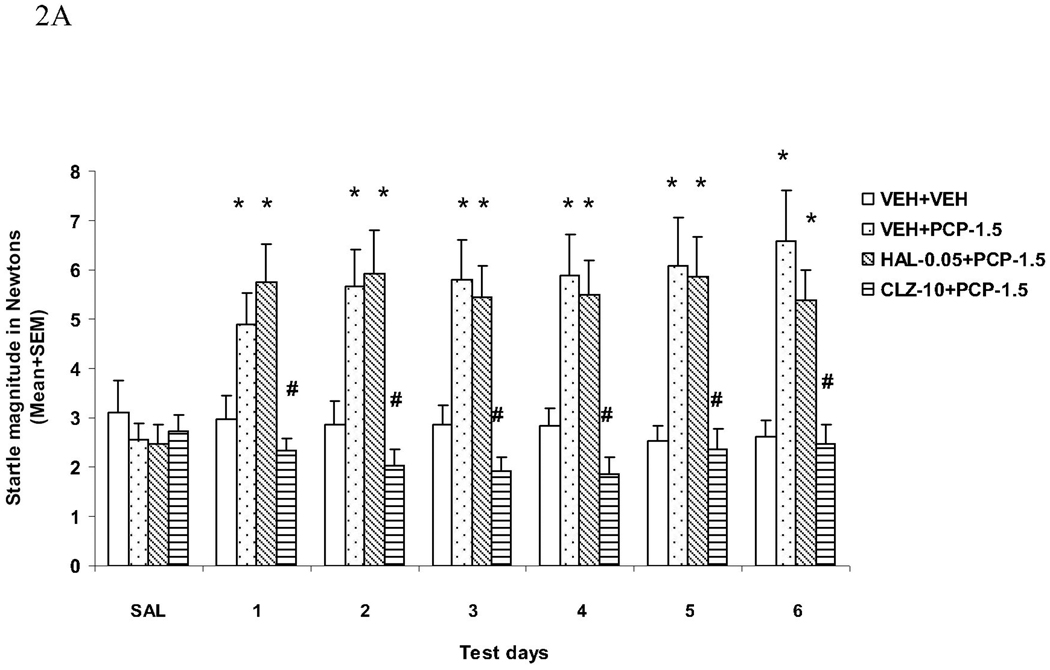
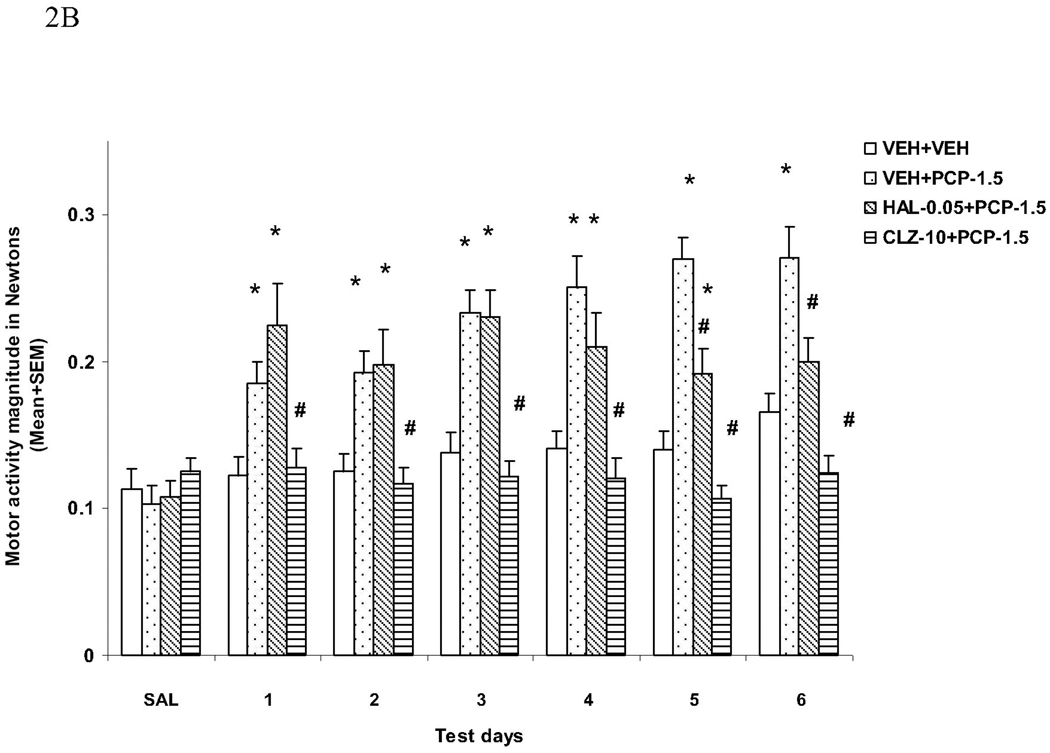
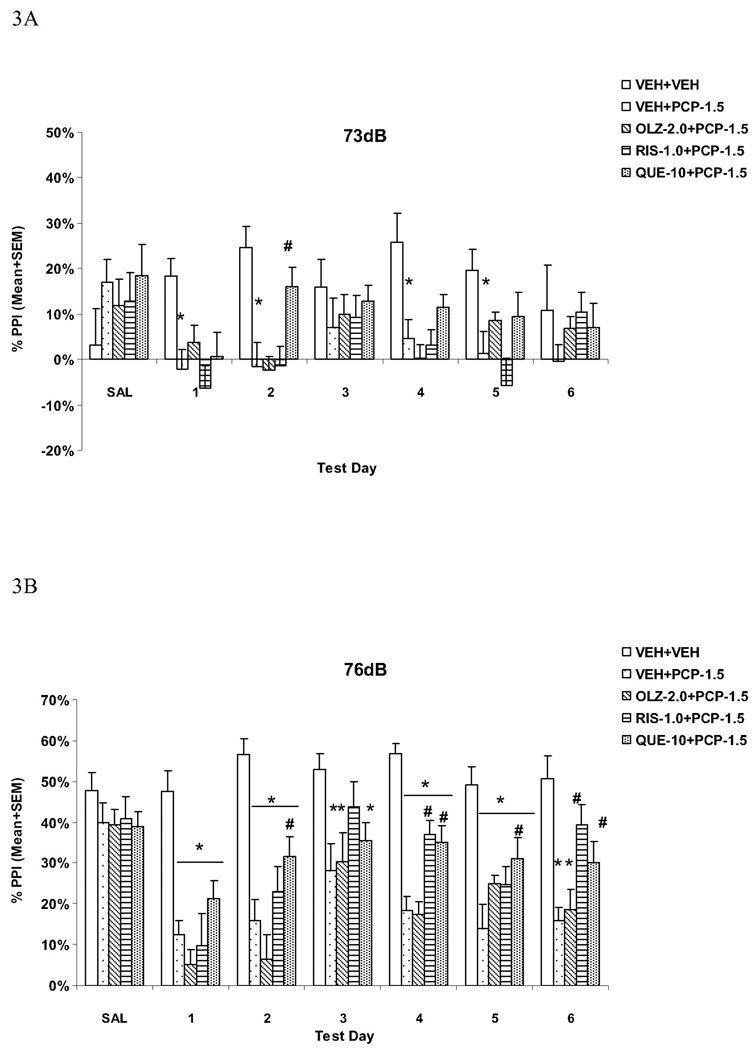
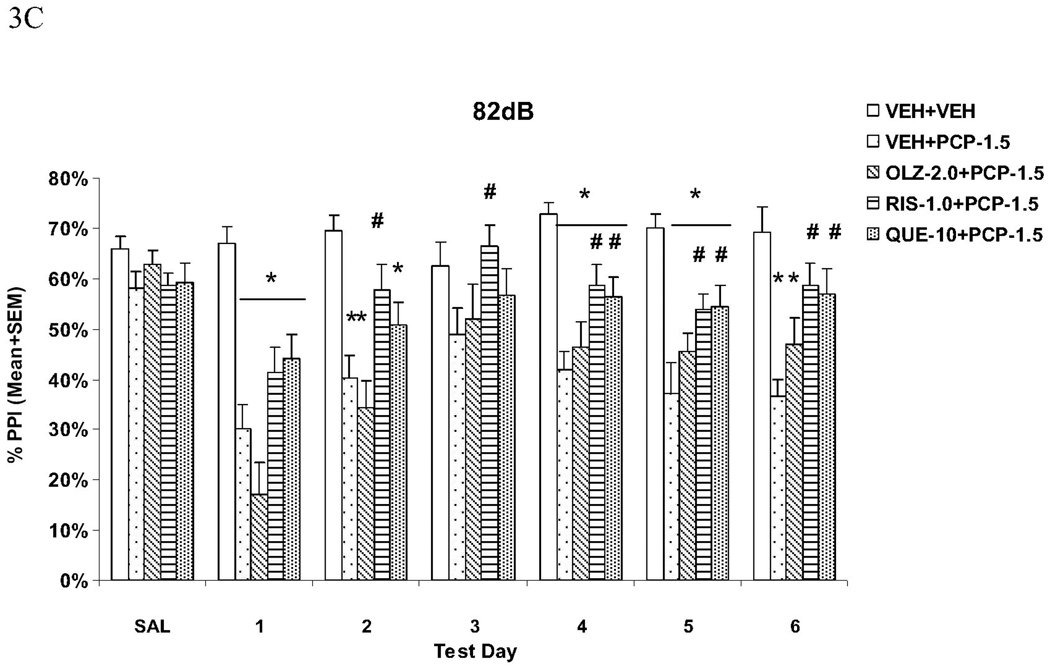
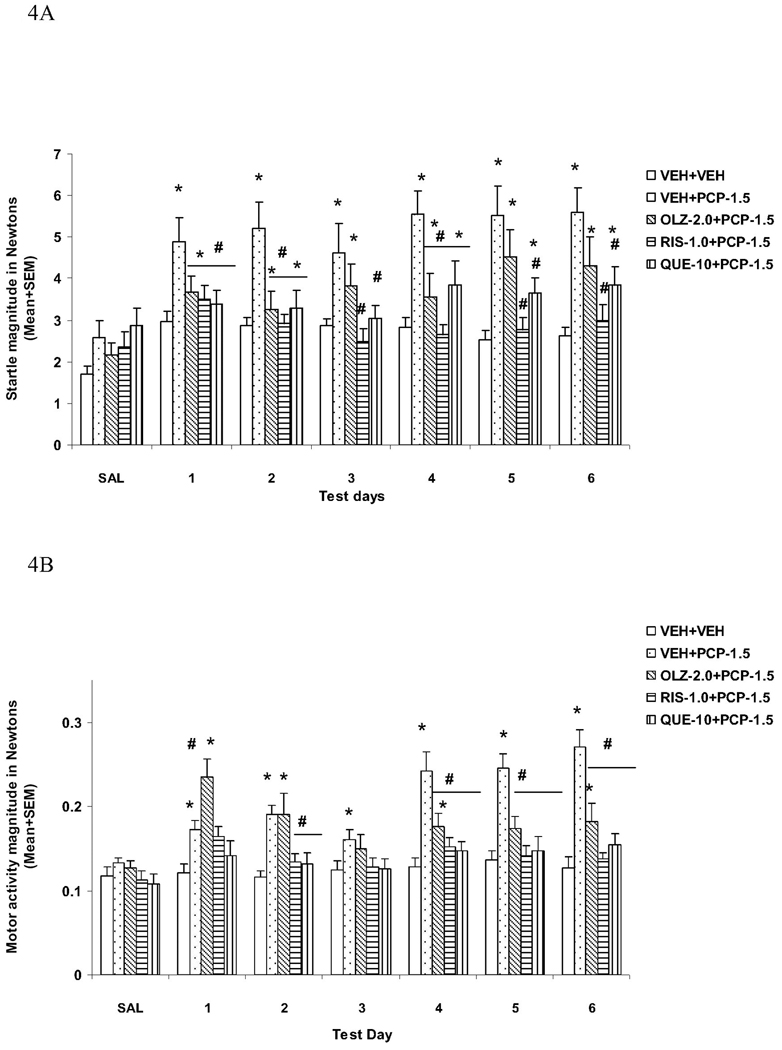
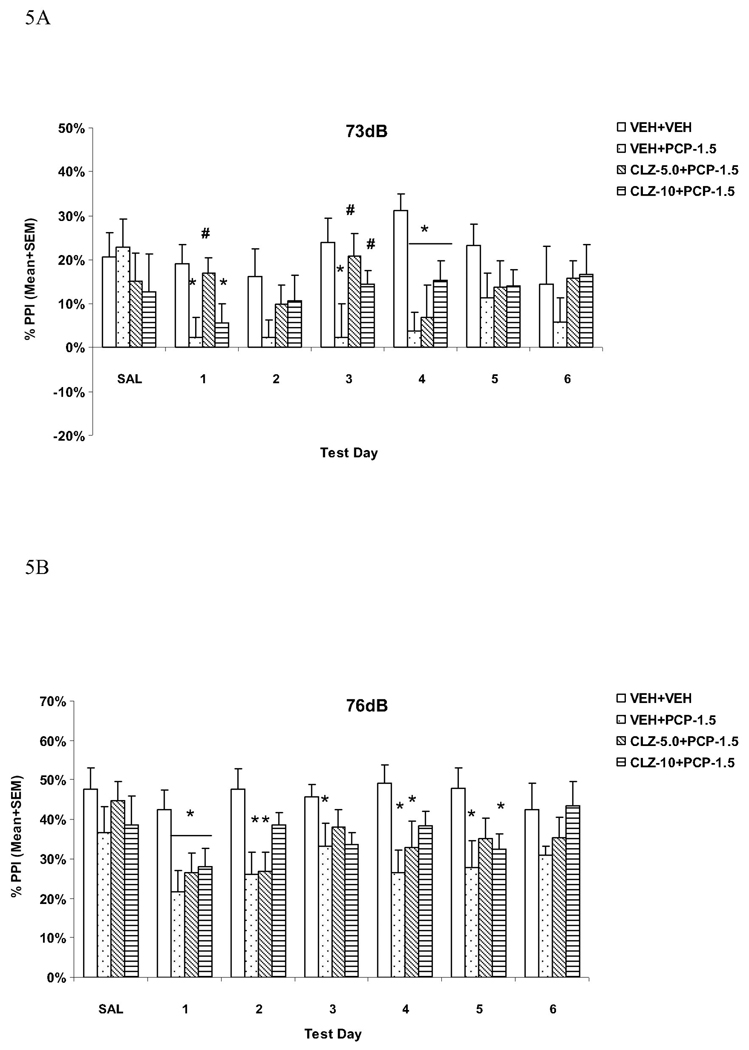
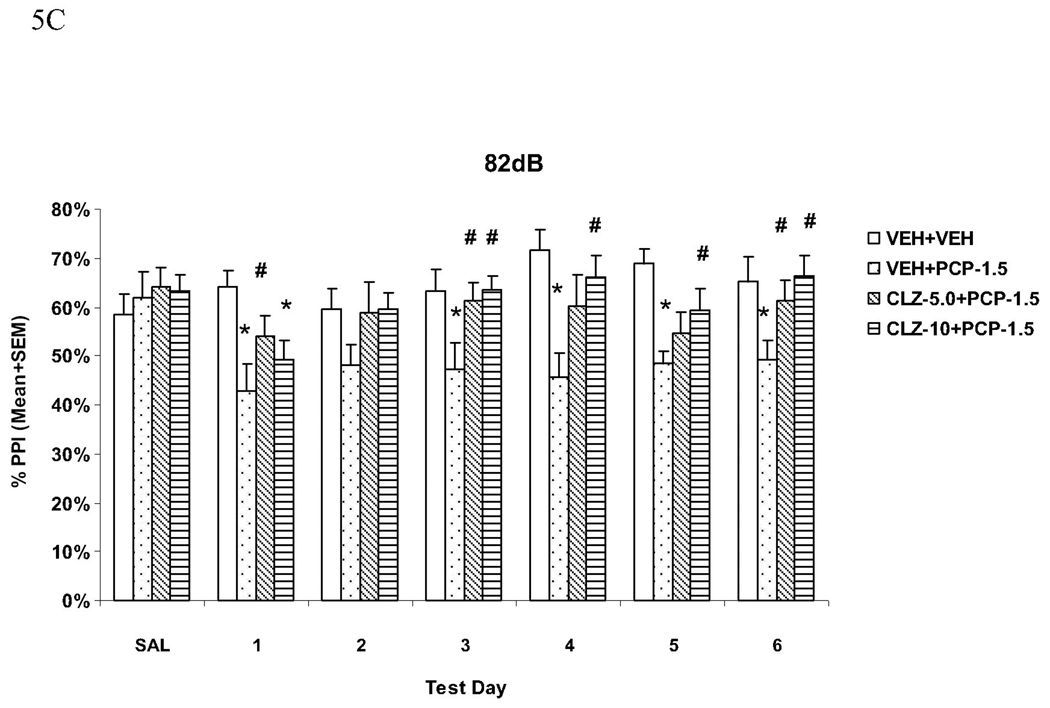
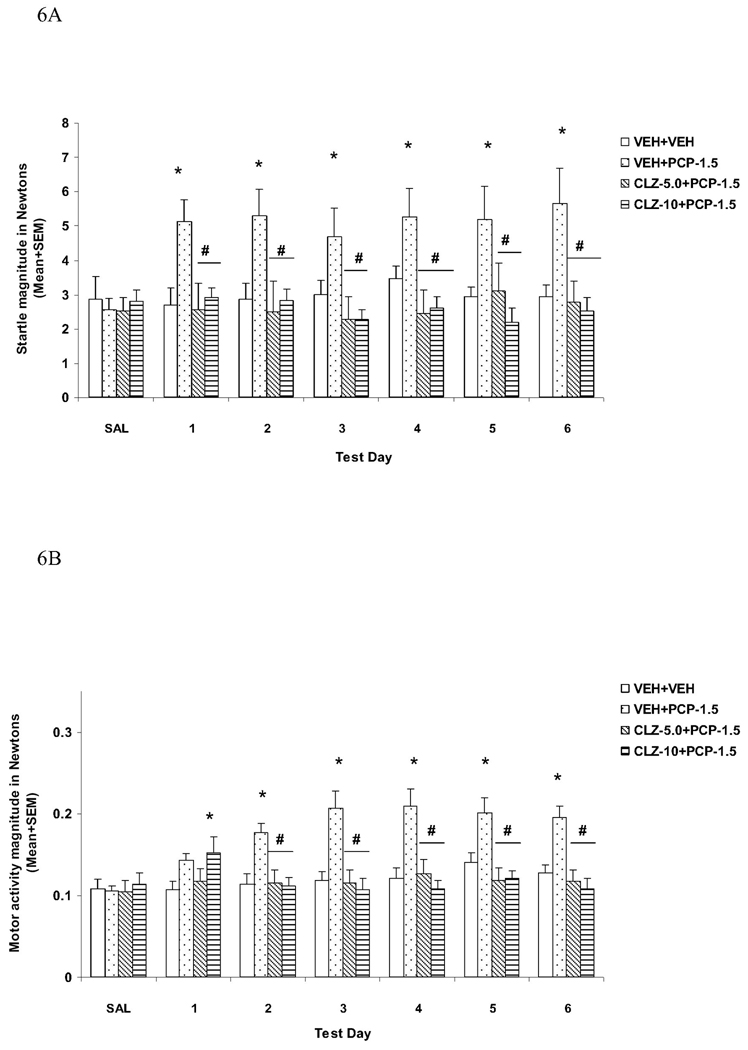
Antagonism of prepulse inhibition (PPI) deficits produced by psychotomimetic drugs has been widely used as an effective tool for the study of the mechanisms of antipsychotic action and identifying potential antipsychotic drugs. Many studies have relied on the acute effect of a single administration of antipsychotics, whereas patients with schizophrenia are treated chronically with antipsychotic drugs. The clinical relevance of acute antipsychotic effect in this model is still an open question. In this study, we investigated the time course of repeated antipsychotic treatment on persistent PPI deficit induced by repeated phencyclidine (PCP) treatment. After a baseline test with saline, male Sprague-Dawley rats were repeatedly injected with either vehicle, haloperidol (0.05mg/kg), clozapine (5.0 or 10.0mg/kg), olanzapine (2.0mg/kg), risperidone (1.0mg/kg) or quetiapine (10mg/kg), followed by PCP (1.5mg/kg, sc) and tested for PPI once daily for 6 consecutive days. A single injection of PCP disrupted PPI and this effect was maintained with repeated PCP injections throughout the testing period. Acute clozapine, but not other antipsychotic drugs, attenuated acute PCP-induced PPI disruption at both tested doses. With repeated treatment, clozapine and quetiapine maintained their attenuation, while risperidone enhanced its effect with a significant reduction of PCP-induced disruption toward the end of treatment period. In contrast, repeated haloperidol and olanzapine treatments were ineffective. The PPI effects of these drugs were more conspicuous at a higher prepulse level (e.g. 82dB) and were dissociable from their effects on startle response and general activity. Overall, the repeated PCP-PPI model appears to be a useful model for the study of the time-dependent antipsychotic effect, and may help identify potential treatments that have a quicker onset of action than current antipsychotics.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Abekawa T, Ito K, Koyama T. Different effects of a single and repeated administration of clozapine on phencyclidine-induced hyperlocomotion and glutamate releases in the rat medial prefrontal cortex at short- and long-term withdrawal from this antipsychotic. Naunyn Schmiedebergs Arch Pharmacol. 2007;375:261–271. - PubMed
-
- Agid O, Kapur S, Arenovich T, Zipursky RB. Delayed-onset hypothesis of antipsychotic action: a hypothesis tested and rejected. Arch Gen Psychiatry. 2003;60:1228–1235. - PubMed
-
- Andersen MP, Pouzet B. Effects of acute versus chronic treatment with typical or atypical antipsychotics on d-amphetamine-induced sensorimotor gating deficits in rats. Psychopharmacology (Berl) 2001;156:291–304. - PubMed
-
- Bakshi VP, Geyer MA. Antagonism of phencyclidine-induced deficits in prepulse inhibition by the putative atypical antipsychotic olanzapine. Psychopharmacology (Berl) 1995;122:198–201. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
