

Effects of antiretroviral therapy on immune function of HIV-infected adults with pulmonary tuberculosis and CD4+ >350 cells/mm3
- PMID: 21402550
- PMCID: PMC3068037
- DOI: 10.1093/infdis/jiq141
Effects of antiretroviral therapy on immune function of HIV-infected adults with pulmonary tuberculosis and CD4+ >350 cells/mm3
Abstract
Background: Human immunodeficiency virus (HIV)-tuberculosis coinfection is associated with heightened immune activation, viral replication, and T cell dysfunction. We compared changes in T cell activation and function between patients receiving concurrent treatment for HIV-tuberculosis coinfection and those receiving treatment for tuberculosis alone.
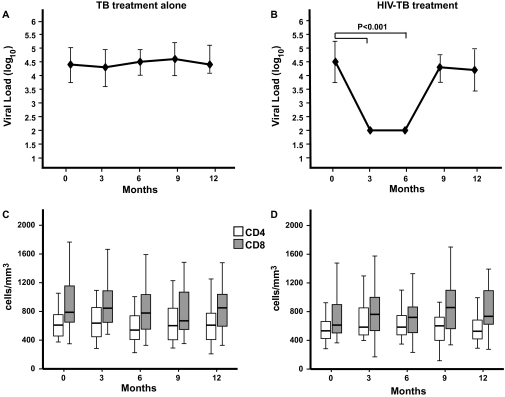
Methods: HIV-infected adults with tuberculosis and CD4(+) T cell counts >350 cells/mm(3) were randomized to receive tuberculosis treatment alone (control arm; n = 36) or 6 months of antiretroviral therapy (ART) concurrent with tuberculosis treatment (intervention arm; n = 38). HIV viral load, T cell subsets, T cell activation, and cytokine production were measured at enrollment and every 3 months for 12 months.
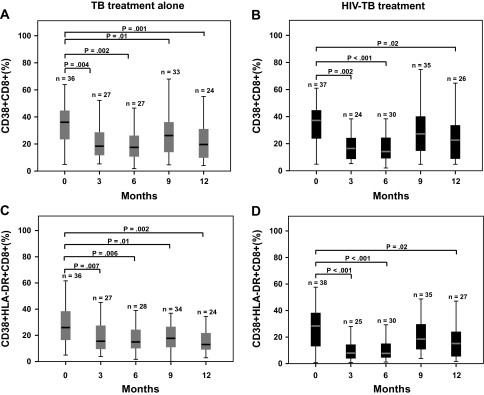
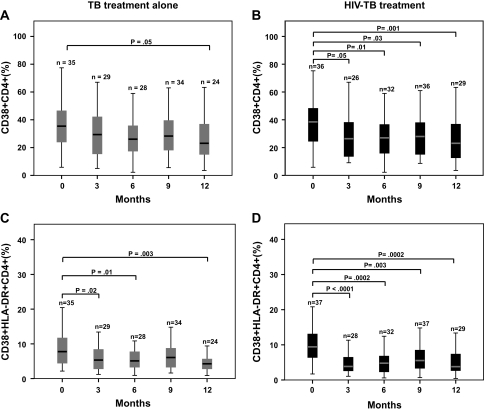
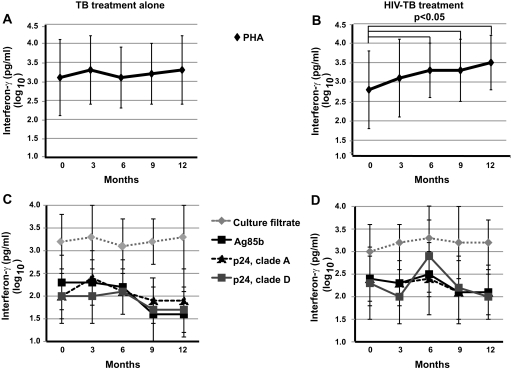
Results: Differences in absolute CD4(+) and CD8(+) T cell counts were not observed between arms. Viral load was reduced while participants received ART; control patients maintained viral load at baseline levels. Both arms had significant reductions in T cell expression of CD38 and HLA-DR. Interferon-γ production in response to mitogen increased significantly in the intervention arm.
Conclusions: In HIV-infected adults with tuberculosis and CD4(+) T cell counts >350 cells/mm(3), both tuberculosis treatment and concurrent HIV-tuberculosis treatment reduce T cell activation and stabilize T cell counts. Concurrent ART with tuberculosis treatment does not provide additional, sustained reductions in T cell activation among individuals with preserved immunologic function.
Figures
References
-
- Daley CL, Small PM, Schecter GF, et al. An outbreak of tuberculosis with accelerated progression among persons infected with the human immunodeficiency virus: an analysis using restriction-fragment-length polymorphisms. N Engl J Med. 1992;326:231–5. - PubMed
-
- Lado Lado FL, Barrio Gomez E, Carballo Arceo E, Cabarcos Ortiz de Barron A. Clinical presentation of tuberculosis and the degree of immunodeficiency in patients with HIV infection. Scand J Infect Dis. 1999;31:387–91. - PubMed
-
- Gilks CF, Brindle RJ, Otieno LS, et al. Extrapulmonary and disseminated tuberculosis in HIV-1-seropositive patients presenting to the acute medical services in Nairobi. AIDS. 1990;4:981–5. - PubMed
-
- Harries AD, Hargreaves NJ, Kemp J, et al. Deaths from tuberculosis in sub-Saharan African countries with a high prevalence of HIV-1. Lancet. 2001;357:1519–23. - PubMed
-
- Korenromp EL, Scano F, Williams BG, Dye C, Nunn P. Effects of human immunodeficiency virus infection on recurrence of tuberculosis after rifampin-based treatment: an analytical review. Clin Infect Dis. 2003;37:101–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
