

Predicting the outcome of ankylosing spondylitis therapy
- PMID: 21402563
- PMCID: PMC3086037
- DOI: 10.1136/ard.2010.147744
Predicting the outcome of ankylosing spondylitis therapy
Erratum in
- Ann Rheum Dis. 2012 Aug;71(8):1434
Abstract
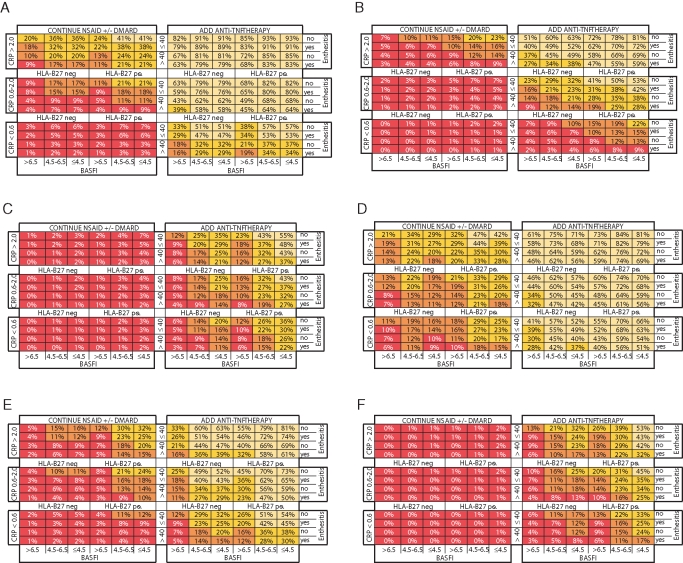
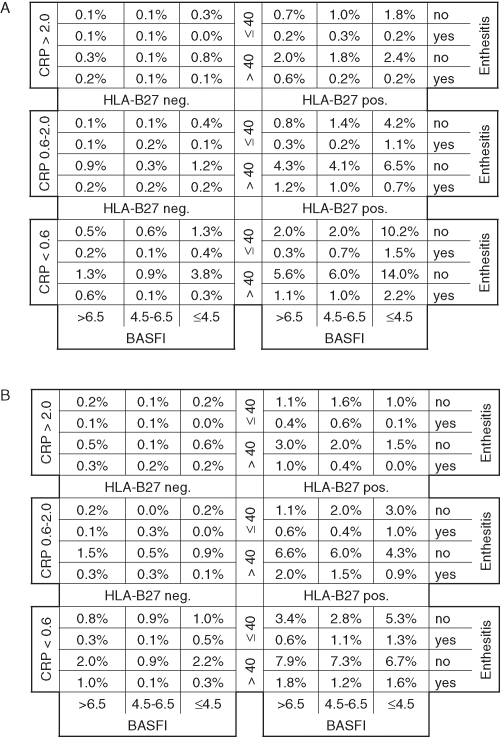
Objectives: To create a model that provides a potential basis for candidate selection for anti-tumour necrosis factor (TNF) treatment by predicting future outcomes relative to the current disease profile of individual patients with ankylosing spondylitis (AS).
Methods: ASSERT and GO-RAISE trial data (n=635) were analysed to identify baseline predictors for various disease-state and disease-activity outcome instruments in AS. Univariate, multivariate, receiver operator characteristic and correlation analyses were performed to select final predictors. Their associations with outcomes were explored. Matrix and algorithm-based prediction models were created using logistic and linear regression, and their accuracies were compared. Numbers needed to treat were calculated to compare the effect size of anti-TNF therapy between the AS matrix subpopulations. Data from registry populations were applied to study how a daily practice AS population is distributed over the prediction model.
Results: Age, Bath ankylosing spondylitis functional index (BASFI) score, enthesitis, therapy, C-reactive protein (CRP) and HLA-B27 genotype were identified as predictors. Their associations with each outcome instrument varied. However, the combination of these factors enabled adequate prediction of each outcome studied. The matrix model predicted outcomes as well as algorithm-based models and enabled direct comparison of the effect size of anti-TNF treatment outcome in various subpopulations. The trial populations reflected the daily practice AS population.
Conclusion: Age, BASFI, enthesitis, therapy, CRP and HLA-B27 were associated with outcomes in AS. Their combined use enables adequate prediction of outcome resulting from anti-TNF and conventional therapy in various AS subpopulations. This may help guide clinicians in making treatment decisions in daily practice.
Conflict of interest statement
Figures

References
-
- Davis JC, Jr, Van Der Heijde D, Braun J, et al. Recombinant human tumor necrosis factor receptor (etanercept) for treating ankylosing spondylitis: a randomized, controlled trial. Arthritis Rheum 2003;48:3230–6 - PubMed
-
- Inman RD, Davis JC, Jr, van der Heijde D, et al. Efficacy and safety of golimumab in patients with ankylosing spondylitis: results of a randomized, double-blind, placebo-controlled, phase III trial. Arthritis Rheum 2008;58:3402–12 - PubMed
-
- van der Heijde D, Dijkmans B, Geusens P, et al. Efficacy and safety of infliximab in patients with ankylosing spondylitis: results of a randomized, placebo-controlled trial (ASSERT). Arthritis Rheum 2005;52:582–91 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
