

Cost implications of the rapid adoption of newer technologies for treating prostate cancer
- PMID: 21402604
- PMCID: PMC3082972
- DOI: 10.1200/JCO.2010.31.1217
Cost implications of the rapid adoption of newer technologies for treating prostate cancer
Abstract
Purpose: Intensity-modulated radiation therapy (IMRT) and laparoscopic or robotic minimally invasive radical prostatectomy (MIRP) are costlier alternatives to three-dimensional conformal radiation therapy (3D-CRT) and open radical prostatectomy for treating prostate cancer. We assessed temporal trends in their utilization and their impact on national health care spending.
Methods: Using Surveillance, Epidemiology, and End Results-Medicare linked data, we determined treatment patterns for 45,636 men age ≥ 65 years who received definitive surgery or radiation for localized prostate cancer diagnosed from 2002 to 2005. Costs attributable to prostate cancer care were the difference in Medicare payments in the year after versus the year before diagnosis.
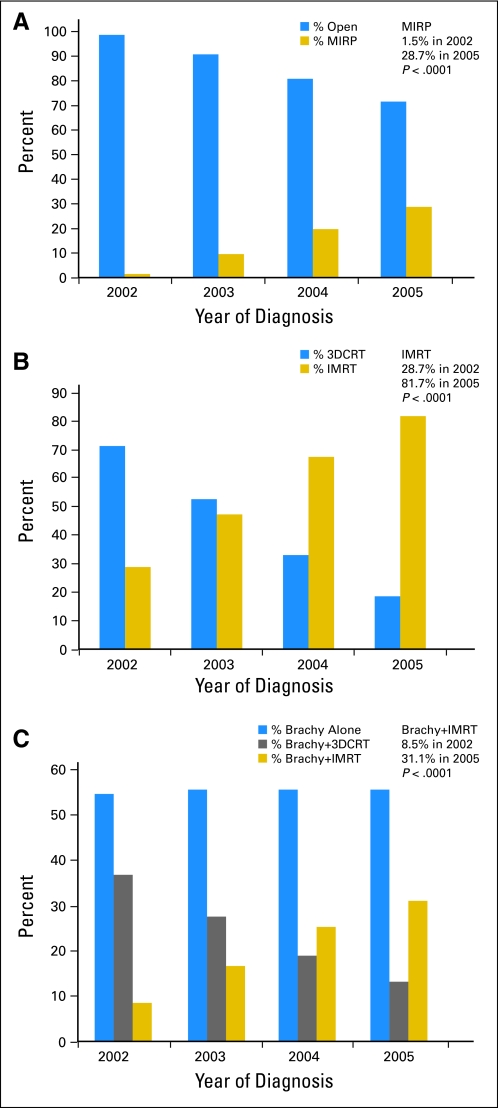
Results: Patients received surgery (26%), external RT (38%), or brachytherapy with or without RT (36%). Among surgical patients, MIRP utilization increased substantially (1.5% among 2002 diagnoses v 28.7% among 2005 diagnoses, P < .001). For RT, IMRT utilization increased substantially (28.7% v 81.7%; P < .001) and for men receiving brachytherapy, supplemental IMRT increased significantly (8.5% v 31.1%; P < .001). The mean incremental cost of IMRT versus 3D-CRT was $10,986 (in 2008 dollars); of brachytherapy plus IMRT versus brachytherapy plus 3D-CRT was $10,789; of MIRP versus open RP was $293. Extrapolating these figures to the total US population results in excess spending of $282 million for IMRT, $59 million for brachytherapy plus IMRT, and $4 million for MIRP, compared to less costly alternatives for men diagnosed in 2005.
Conclusion: Costlier prostate cancer therapies were rapidly and widely adopted, resulting in additional national spending of more than $350 million among men diagnosed in 2005 and suggesting the need for comparative effectiveness research to weigh their costs against their benefits.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
The war on cancer: progress at what price?J Clin Oncol. 2011 Apr 20;29(12):1503-4. doi: 10.1200/JCO.2010.34.2758. Epub 2011 Mar 14. J Clin Oncol. 2011. PMID: 21402613 No abstract available.
-
Prostate cancer: What is the cost of modern cancer treatment?Nat Rev Urol. 2011 Jun 14;8(7):354. doi: 10.1038/nrurol.2011.89. Nat Rev Urol. 2011. PMID: 21670753 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Leonhardt D. In Health Reform, a Cancer Offers an Acid Test. The New York Times. 2009
-
- Bolenz C, Gupta A, Hotze T, et al. Cost comparison of robotic, laparoscopic, and open radical prostatectomy for prostate cancer. Eur Urol. 57:453–458. - PubMed
-
- Cahlon O, Hunt M, Zelefsky MJ. Intensity-modulated radiation therapy: Supportive data for prostate cancer. Semin Radiat Oncol. 2008;18:48–57. - PubMed
-
- Warren JL, Klabunde CN, Schrag D, et al. Overview of the SEER-Medicare data: Content, research applications, and generalizability to the United States elderly population. Med Care. 2002;40:IV-3-18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
