

Clustering of opioid prescribing and opioid-related mortality among family physicians in Ontario
- PMID: 21402956
- PMCID: PMC3056701
Clustering of opioid prescribing and opioid-related mortality among family physicians in Ontario
Abstract
Objective: To examine whether variation in prescribing at the level of the individual physician is associated with opioid-related mortality.
Design: A population-based cross-sectional analysis linking prescription data with records from the Office of the Chief Coroner.
Setting: The province of Ontario. Participants Family physicians in Ontario and Ontarians aged 15 to 64 who were eligible for prescription drug coverage under the Ontario Public Drug Program.
Main outcome measures: Variation in family physicians' opioid prescribing and opioid-related mortality among their patients.
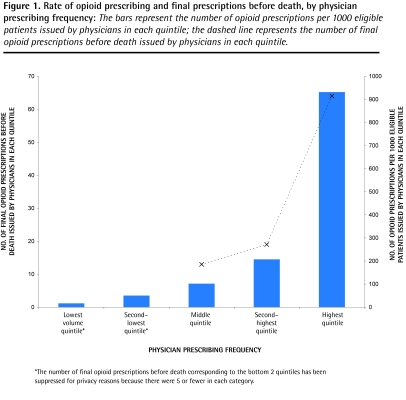
Results: The 20% of family physicians (n = 1978) who prescribed opioids most frequently issued opioid prescriptions 55 times more often than the 20% who prescribed opioids least frequently. Family physicians in the uppermost quintile also wrote the final opioid prescription before death for 62.7% of public drug plan beneficiaries whose deaths were related to opioids. Physician characteristics associated with greater opioid prescribing were male sex (P = .003), older age (P < .001), and a greater number of years in practice (P < .001).
Conclusion: Opioid prescribing varies remarkably among family physicians, and opioid-related deaths are concentrated among patients treated by physicians who prescribe opioids frequently. Strategies to reduce opioid-related harm should include efforts focusing on family physicians who prescribe opioids frequently.
Objectif: Vérifier si le fait pour un médecin donné de faire plus ou moins de prescriptions d’opiacés est associé au nombre de décès lié aux opiacés.
Type d‘étude: Analyse transversale de nature démographique sur le lien entre les données relatives aux ordonnances et les registres du bureau du coroner en chef.
Contexte: La province d’Ontario.
Participants: Médecins de famille d’Ontario et patients ontariens entre 15 et 64 ans qui étaient admissibles au programme de médicaments d’ordonnance conformément à l’Ontario Public Drug Program.
Principaux paramètres à l’étude: Variations, chez les médecins de famille, dans la prescription d’opiacés et les décès reliés aux opiacés parmi leurs patients.
Résultats: Parmi les médecins de famille, les 20 % (n = 1978) qui prescrivaient des opiacés le plus fréquemment en prescrivaient 55 fois plus souvent que les 20 % qui en prescrivaient le moins souvent. Les médecins qui faisaient le plus de prescriptions avaient aussi fait la dernière prescription précédant la mort pour 62,7 % des bénéficiaires du programme public de médicaments dont la mort était reliée aux opiacés. Les caractéristiques des médecins qui faisaient le plus de prescriptions d’opiacés étaient les suivantes : sexe masculin (P = ,003), plus âgés (P < ,001) et plus grand nombre d’années de pratique (P < ,001).
Conclusion: La prescription d’opiacés varie beaucoup entre les médecins de famille, et les décès reliés aux opiacés sont concentrés parmi les patients traités par les médecins qui prescrivent plus souvent des opiacés. Les stratégies pour réduire les dangers associés aux opiacés devraient cibler principalement les médecins qui prescrivent fréquemment des opiacés.
Figures
Comment in
-
Opioids, pain, and personality: the story of a substitute physician.Can Fam Physician. 2011 Mar;57(3):271-2. Can Fam Physician. 2011. PMID: 21520666 Free PMC article. No abstract available.
-
Mind the gap.Can Fam Physician. 2011 May;57(5):530-1; author reply 537-9. Can Fam Physician. 2011. PMID: 21571710 Free PMC article. No abstract available.
-
Misleading conclusions.Can Fam Physician. 2011 May;57(5):530; author reply 537-9. Can Fam Physician. 2011. PMID: 21571711 Free PMC article. No abstract available.
-
Opioid prescribing--a matter of ethics.Can Fam Physician. 2011 May;57(5):531-2; discussion 532; author reply 537-9. Can Fam Physician. 2011. PMID: 21571712 Free PMC article. No abstract available.
-
Treating patients versus numbers.Can Fam Physician. 2011 May;57(5):532-5; author reply 537-9. Can Fam Physician. 2011. PMID: 21571713 Free PMC article. No abstract available.
-
The opioid crisis in North America.Can Fam Physician. 2011 May;57(5):536; author reply 537-9. Can Fam Physician. 2011. PMID: 21571715 Free PMC article. No abstract available.
-
Clustering of opioid prescribing--what is really going on?Can Fam Physician. 2011 May;57(5):535-6; author reply 537-9. Can Fam Physician. 2011. PMID: 21642735 Free PMC article. No abstract available.
References
-
- Warner M, Chen LH, Makuc DM. Increase in fatal poisonings involving opioid analgesics in the United States, 1999–2006. Atlanta, GA: Centres for Disease Control and Prevention; 2009. Available from: www.cdc.gov/nchs/data/databriefs/db22.htm. Accessed 2010 Nov 11. - PubMed
-
- Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med. 2003;349(20):1943–53. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources