

Long-term renal outcomes of patients with type 1 diabetes mellitus and microalbuminuria: an analysis of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications cohort
- PMID: 21403038
- PMCID: PMC3085024
- DOI: 10.1001/archinternmed.2011.16
Long-term renal outcomes of patients with type 1 diabetes mellitus and microalbuminuria: an analysis of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications cohort
Abstract
Background: Microalbuminuria is a common diagnosis in the clinical care of patients with type 1 diabetes mellitus. Long-term outcomes after the development of microalbuminuria are variable.
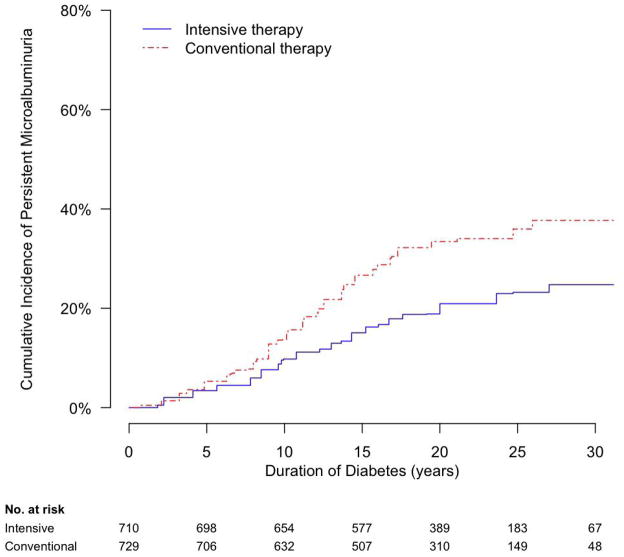
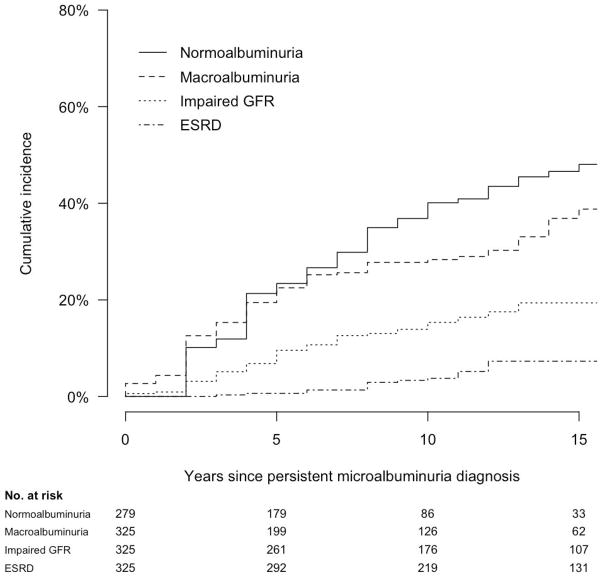
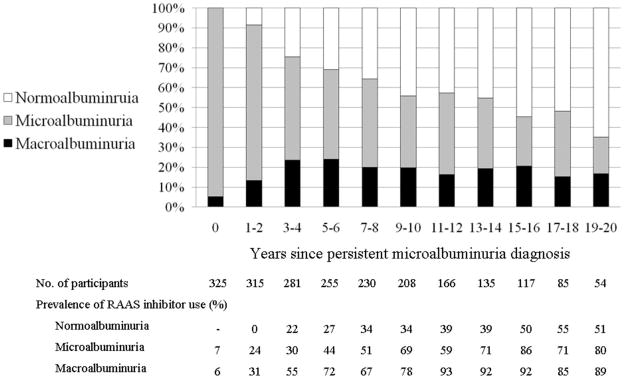
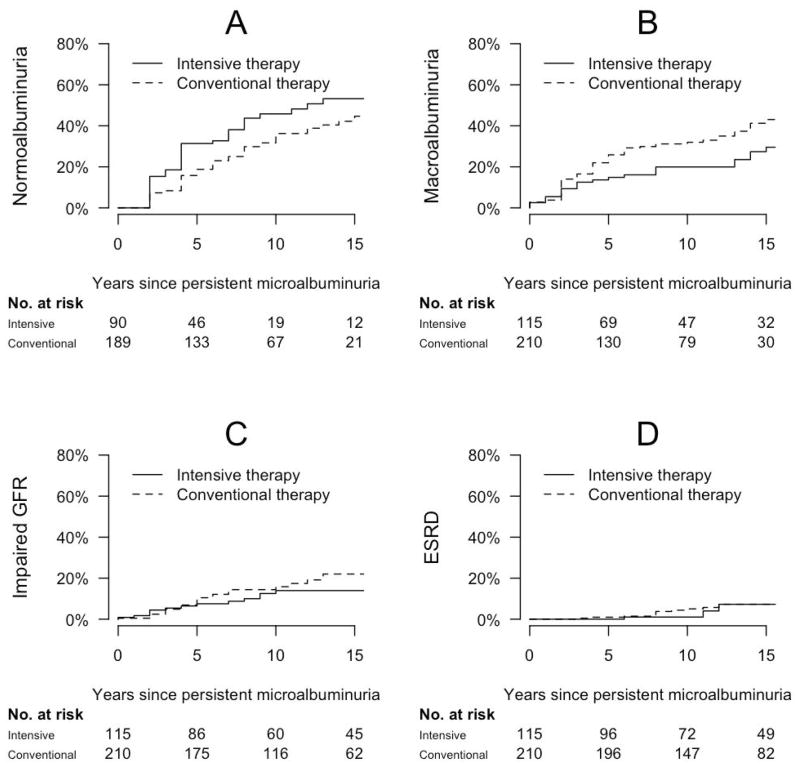
Methods: We quantified the incidence of and risk factors for long-term renal outcomes after the development of microalbuminuria in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) study. The DCCT randomly assigned 1441 persons with type 1 diabetes to intensive or conventional diabetes therapy, and participants were subsequently followed up during the observational EDIC study. During the DCCT/EDIC study, 325 participants developed incident persistent microalbuminuria (albumin excretion rate, ≥30 mg/24 h at 2 consecutive study visits). We assessed their subsequent renal outcomes, including progression to macroalbuminuria (albumin excretion rate, ≥300 mg/24 h at 2 consecutive visits), impaired glomerular filtration rate (estimated glomerular filtration rate, <60 mL/min/1.73 m(2) at 2 consecutive study visits), end-stage renal disease, and regression to normoalbuminuria (albumin excretion rate, <30 mg/24 h at 2 consecutive visits).
Results: The median follow-up period after persistent microalbuminuria diagnosis was 13 years (maximum, 23 years). Ten-year cumulative incidences of progression to macroalbuminuria, impaired glomerular filtration rate, end-stage renal disease, and regression to normoalbuminuria were 28%, 15%, 4%, and 40%, respectively. Albuminuria outcomes were more favorable with intensive diabetes therapy, lower glycated hemoglobin level, absence of retinopathy, female sex, lower blood pressure, and lower concentrations of low-density lipoprotein cholesterol and triglycerides. Lower glycated hemoglobin level, absence of retinopathy, and lower blood pressure were also associated with decreased risk of impaired glomerular filtration rate.
Conclusions: After the development of persistent microalbuminuria, progression and regression of kidney disease each commonly occur. Intensive glycemic control, lower blood pressure, and a more favorable lipid profile are associated with improved outcomes.
©2011 American Medical Association. All rights reserved.
Figures
Comment in
-
ACP Journal Club. 13-year renal outcomes varied in patients with type 1 diabetes and new-onset microalbuminuria.Ann Intern Med. 2011 Jul 19;155(2):JC1-13. doi: 10.7326/0003-4819-155-2-201107190-02013. Ann Intern Med. 2011. PMID: 21768579 No abstract available.
-
Long-term renal outcomes of patients with type 1 diabetes mellitus and microalbuminuria: an analysis of the DCCT/EDIC cohort.Arch Intern Med. 2011 Sep 26;171(17):1596; author reply 1597. doi: 10.1001/archinternmed.2011.413. Arch Intern Med. 2011. PMID: 21949179 No abstract available.
References
-
- Parving HH, Oxenboll B, Svendsen PA, Christiansen JS, Andersen AR. Early detection of patients at risk of developing diabetic nephropathy. A longitudinal study of urinary albumin excretion. Acta Endocrinol (Copenh) 1982 Sep;100(4):550–555. - PubMed
-
- Viberti GC, Hill RD, Jarrett RJ, Argyropoulos A, Mahmud U, Keen H. Microalbuminuria as a predictor of clinical nephropathy in insulin-dependent diabetes mellitus. Lancet. 1982 Jul 26;1(8287):1430–1432. - PubMed
-
- Mogensen CE. Microalbuminuria predicts clinical proteinuria and early mortality in maturity-onset diabetes. N Engl J Med. 1984 Feb 9;310(6):356–360. - PubMed
-
- Effect of intensive therapy on the development and progression of diabetic nephropathy in the Diabetes Control and Complications Trial. The Diabetes Control and Complications (DCCT) Research Group. Kidney Int. 1995 Jun;47(6):1703–1720. - PubMed
